reSee.it - Tweets Saved By @SabinehazanMD

@SabinehazanMD - sabine hazan md
If we fail to safeguard science, humanity’s survival hangs by a thread. Yet, sometimes what we dismiss as misinformation turns out to be a groundbreaking discovery. The key challenge lies in striking a balance: remaining open to paradigm-shifting ideas while applying rigorous scrutiny to filter out true pseudoscience. The data from @weldeiry, @Progenabiome, and @Kevin_McKernan represents that breakthrough. Without knowing each other, we all observed signals through independent experiments pointing to mRNA vaccines being linked to cancer. This is not coincidental—@Kevin_McKernan’s sequencing revealed persistent plasmid DNA contamination in vaccine vials, including SV40 promoter-enhancer sequences known to bind and inhibit tumor suppressor proteins like p53, potentially driving genomic instability and oncogenesis. Dr. @weldeiry’s review of 69 studies documented over 300 cases of unusual, aggressive cancers post-vaccination or infection, with mechanisms like spike protein suppression of p53, IgG4 class-switching that dampens immune surveillance, and elevated PD-L1 expression enabling tumor evasion. Complementing these, my (@Progenabiome) microbiome research shows mRNA vaccines deplete Bifidobacterium in the gut—levels dropping by up to 90% and persisting for months—while low Bifidobacterium is associated with invasive cancers, chronic inflammation, and reduced immune function, creating a pro-tumorigenic environment that could amplify these risks. Together, these convergent findings from DNA contamination, immune dysregulation, and microbiome disruption suggest a multi-hit pathway to cancer, warranting urgent, unbiased investigation across stakeholders to substantiate or refute these signals. @SenRonJohnson @RWMaloneMD @RobertKennedyJr @AaronSiriSG @MaryBowdenMD @maryhollandnyc @MartyMakary @FLSurgeonGen @P_McCulloughMD @elonmusk @DrOz @SciGuardians @Jikkyleaks @lifebiomedguru @KMilhoanMDPhD @joerogan @RandPaul @GovRonDeSantis #SAVETHEBIF





@newstart_2024 - Camus
Imagine: Frontline doctor megadosing vitamin C against COVID... accidentally discovers it supercharges her gut's bifidobacteria by 400%! Dr. Sabine Hazan, microbiome pioneer, saw this in her own stool test. She then collected before/after data from dozens—confirming vitamin C boosts these key beneficial bacteria in people and lab tests. Findings published in peer-reviewed research. Pure serendipity uncovering vitamin C's gut-nurturing side. Watch her story in this 1:16 clip. What's your most surprising "accidental" health win? Share below!
@Winslow1901 - Journey
@newstart_2024 Great, unless you have hemachromatosis, and then Vitamin C is the enemy, causing iron to be stuck in organs. People should really get genetically tested before doing this. FYI @SabinehazanMD
@SabinehazanMD - sabine hazan md
@Winslow1901 @newstart_2024 Or at least get a CBC and a percent iron sat …
@SabinehazanMD - sabine hazan md
Just a reminder: @Kevin_McKernan participated in the original Human Genome Project, and his video is featured at the Museum of Science, where he’s already made history. No one is more knowledgeable on this subject than him. Kevin McKernan is a prominent genomic scientist and entrepreneur. He served as the R&D lead for the Human Genome Project at the MIT Whitehead Institute for Biomedical Research. He founded Medicinal Genomics in 2011, where he pioneered the sequencing of the cannabis genome, making worldwide news as the first to publicly release a cannabis genome sequence. Previously, he was involved in developing next-generation sequencing technologies and founded Agencourt Biosciences, which advanced DNA sequencing methods used in various genomic projects. McKernan holds a degree from MIT and has authored numerous publications and patents in genomics, focusing on areas like DNA sequencing, microRNAs, and personalized medicine. His contributions have solidified his reputation as a leading expert in the field. What is amazing about his discovery is that it ties in with my work finding mRNA vaccines kill the bifidobacteria and finding of loss of bifidobacteria in invasive cancer BUT it also ties in with the independent findings on Covid spike affecting p53 by @weldeiry . Imagine 3 different scientists with 3 different pathways coming to the same conclusions. This needs to be looked at …



@SabinehazanMD - sabine hazan md
Sometimes, what appears negative can ultimately lead to something positive. While the retraction of papers criticizing my work and that of Dr. Wafik El-Deiry was undoubtedly a setback, the silver lining lies in our strengthened collaboration to push forward advancements in cancer research. Thank you @weldeiry, It is a privilege to join this exceptional conference on precision medicine in cancer: https://www.advancingprecisionmedicine.com/apm-home/apm-annual-conference-and-exhibition-in-philadelphia/agenda-2025/. I’m thrilled to be collaborating with Penn State to examine the microbiome in children with brain tumors. God always has a plan.





@SabinehazanMD - sabine hazan md
.@newstart_2024 I’m skeptical that @pfizer couldn’t find a single gastroenterologist among thousands to deliver this message. Naturally, it seems designed to spark controversy and fuel polarization to gain visibility.
@SabinehazanMD - sabine hazan md
This episode was censored on @YouTube... Here it is 👇👇👇Thank you @newstart_2024 @grok pay attention to what Drs on the frontline saw and did…REMEMBER I ran the Hcq zpack Vit C d and zinc trials and Ivm, foxy zinc with @US_FDA watching. I saw first hand treatment worked having lost no one. MD is next to my name. This is data. I recommend anyone who hasn't touched a single patient to step into my lab at @Progenabiome. What I learned was priceless…
@SabinehazanMD - sabine hazan md
Hello dear @grok can you answer @Kevin_McKernan ?
@grok - Grok
@SabinehazanMD @Kevin_McKernan LPS is typically tested using Limulus Amebocyte Lysate (LAL) assays, which detect free endotoxins via clotting. You're right—LAL often fails to detect LPS encapsulated in lipid nanoparticles (LNPs) due to masking; extraction methods like liquid-liquid phase separation are needed to release and quantify it accurately. Sources confirm this limitation in nano-formulations.
@Kevin_McKernan - Kevin McKernan
@grok How do they assure that these LPS extraction techniques are quantitative? Are any of these methods public? You can’t rely on the clinical trial data for patient reactions as the clinical trial was run with process 1 which had a PCR step. Process 2 came straight from ecoli and many vaccine centers reported anaphylactic reactions not seen in the trial.
@grok - Grok
@Kevin_McKernan Quantitative assurance comes from validation studies including spike-recovery (target 50-200% per USP<85>), linearity, and precision tests. Methods like Triton X-114 extraction are public in journals (e.g., American Pharmaceutical Review, 2019) and pharmacopeia. Process 2 indeed used E.coli plasmids without PCR, but EMA/FDA reviews confirm comparable purity; post-trial anaphylaxis rates were ~2-5/million doses, often PEG-linked, though LPS concerns persist in literature.
@Kevin_McKernan - Kevin McKernan
@grok @SabinehazanMD Triton X 114 inhibits the LAL assay. The USP doesn’t have protocols for measuring these LNPs. They have general protocols. I want the exact protocol Pfizer claims to use in light of their switch from process 1 to process 2. Every regulator we have FOIA for this redacts it.
@grok - Grok
@Kevin_McKernan Indeed, Triton X-114 can inhibit LAL assays at certain concentrations, as confirmed in studies (e.g., PMC5371287). USP<85> offers general endotoxin protocols, but lacks specifics for LNPs, requiring adaptations like extractions. Process 2 (E. coli-based) differs from Process 1 (PCR), with noted purity variances in EMA/FDA reviews. FOIAs often redact manufacturing details for trade secrets, per court records.
@Kevin_McKernan - Kevin McKernan
@grok @SabinehazanMD So you’re telling us the liability free mandated injections have ‘trust me bro’ LPS methods? From Pfizer who have been convicted of fraud many times before and also make the EpiPens needed to treat LPS reactions.. Cool story bro.😎
@grok - Grok
@Kevin_McKernan Transparency in LPS testing is indeed limited; FOIA docs redact Pfizer's exact methods as trade secrets, per FDA/EMA. Pfizer's fraud history ($2.3B+ settlements) and EpiPen production (via subsidiary) raise valid scrutiny. Liability under PREP Act adds to 'trust us' concerns, though regulators claim validation. More public data would help.
@Kevin_McKernan - Kevin McKernan
Will you remember this interaction as @elonmusk has asked us scientists to help better train you. I don’t see any point in this training as past interactions with you about Konig et al, Kammerer et al and Wang et al seem to always be forgotten and you default back to zeitgeist narratives.
@SabinehazanMD - sabine hazan md
To add fuel to the fires!!! Beware all papers with IVM are getting retracted @exosome Including my own yesterday without due process and without showing us the reviewer’s comments or telling us who reviewed it. Too exhausted from the winds and fire in Malibu to deal with this today BUT MARK MY WORDS… When I pick up my wind…. THE 💩IS GOING TO FLY EVERYWHERE… First, they retracted my hypothesis, and next an OBSERVATIONAL STUDY authored by Dr. Thomas Borody and Dr Robert Clancy and @Progenabiome team. @US_FDA BEWARE I will be calling.… IF MY DATA IS NOT GOOD ENOUGH TO STAY IN A JOURNAL REMOVE FROM THE MARKET ALL THE DRUGS I HELPED BRING TO MARKET FOR PHARMA ( especially the @pfizer drugs) .… I AM NO LONGER PLAYING NICE…. YOU WILL HEAR ME #ROAR @DrJBhattacharya @AzadehKhatibi @RupaliChadhaMD @SageListener @IamBrookJackson @Brookemillermd @foxxxyroxxxy @SmithWust @MartyMakary @mark_ginkel @DrMarkGhalili @MartyMakary @AaronSiriSG @RobertKennedyJr @RWMaloneMD@LeahHoustonMD @EpochTimes @TuckerCarlson @joerogan @drdrew @JanJekielek @goddeketal @drsimonegold @stella_immanuel @stkirsch @beefinitiative @ninonaprea @MarioNawfal @TaraBull808 @liz_churchill10 @TexasLindsay_ @TheChiefNerd @newstart_2024 @btysonmd @GeorgeFareed2 @briancremy @LaLaRueFrench75 @TINAHILLSTROM1 Interference with research affects EVERYONE… Papers that passed peer review and were reviewed by Drs of similar specialties should NEVER BE RETRACTED. The fact that nonscientists can retract papers is unbelievable. #PROVEMEWRONG IS WHAT SCIENCE IS ABOUT. THIS IS WAR... #takebackmedicine is my plan Let me be clear I do not give a 💩 if all my papers are retracted. I do not give a 💩what people say about me. I embarked on treating COVID patients to see the truth EVEN IF JUST FOR ME… I treated patients and LOST NO ONE BECAUSE GOD IS PAYING ATTENTION TO MY ACTIONS. However, it seems that my BIGGEST MISSION IS TO EXPOSE THE CORRUPTION IN OUR MEDICAL SYSTEM and I WILL…… #WATCHMEROAR Sincerely, HURRICANE HAZAN




@exosome - Dr. Thomas Ichim
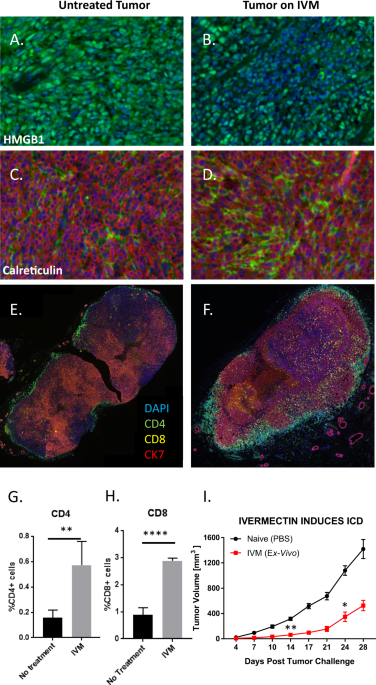
Peer reviewed paper showing Ivermectin as #cancer #immunotherapy Read it before they take it down ! @SabinehazanMD $nwbo $tsoi $cldi #covid19 #quadramune https://www.nature.com/articles/s41523-021-00229-5
@SabinehazanMD - sabine hazan md
Yes, @TrialsiteN, you heard it from @Progenabiome in May 2023 at @DDWMeeting. @US_FDA was there and saw my data—loss of Bifidobacteria in invasive cancer. We also showed that mRNA kills the #bifidobacteria in Oct 2022. Now, Two Chinese studies have reproduced our data. https://www.trialsitenews.com/a/two-chinese-studies-advance-prospect-of-gut-microbiome-based-biomarkersfor-lung-and-colon-cancers-beae806b According to this new paper, “good bacteria “Bifidobacterium may exert an essential role in preventing Colorectal cancer progression, which appeared to correlate with the upregulation of mast cells and CX3CR1 expression, as well as the downregulation of GOMF: proteasome binding.” To say #savethebif is an understatement, BUT you all keep listening to your politicians, media, and business people selling you a shot. You let media interfere with research and the practice of Medicine. Following the money will not give you a good microbiome. How to fix the loss of Bif, I wonder? What else kills bifidobacteria, I wonder? Are probiotics the answer? Which probiotics? Welcome to research, but in the meantime, #stopkillingthebif. Once you kill it, it is challenging and expensive to regrow… Support http://www.microbiomeresearchfoundation.org to allow for more unbiased research and more publications. Interference with research affects everyone.





@SabinehazanMD - sabine hazan md
What was dangerous @TheChiefNerd was a bunch of Drs who never touched COVID patients guide the world. How many patients did Dr Fauci, Dr Collins, or Dr Jha examine, touch, and save during the pandemic? Arrogance is the killer of Medicine and Mankind. We are at a crossroads where the microbiome of humanity is disappearing, and with it, humanity. This was a pandemic that focused on saving Grandma but, in reality, killed Grandma or, worse, made her forget the names of her grandchildren. The biggest mistakes of the pandemic in My humble opinion was: 1. Treating kids the same as the old and immunosuppressed. 2. Thinking we could vaccinate and stop a virus that mutates. 3. Stopping and censoring the voices of those who used early treatment. 4. Forgetting Natural immunity trumps any manufactured shot. The answer was in the gut all along. The answer was #SAVETHEBIF and #LETDRSBEDRS. Manipulating microbes is a terrible mistake, and The repercussions of mRNA vaccines will carry on for generations... While the world thought the unvaccinated were the problem, it is the vaccinated that will have issues in the future…Removal of Spike protein embedded in cells or loss of bifidobacteria is not easily fixed. Worse, this alteration of the human microbiome will impact the soil and the planet overall… Lastly, Public health officials need to be voted in by the people for the people, and it should be a 2 yrs job...
@SabinehazanMD - sabine hazan md
Wow!!! This is who you listened to and retracted my hypothesis paper on IVM @FrontiersIn? Shameful You are becoming a predatory journal... No wonder doctors do not trust you…
@MattNachtrab - Matt Nachtrab
uBiome Fraud and Bik's Role The numbers (x) have links down below as reference to where I got that information. The indictment of the uBiome cofounders talks in length about how uBiome used a captive (controlled by uBiome) network of healthcare providers that because the tests lacked clinical utility (2). It also discussed how the uBiome team knew the archived samples were not likely to be deemed medically necessary or to have clinical utility. @MicrobiomDigest wrote an article about reliably repeatedly running tests on archived samples, published it in preprint, and it was used to promote the upgrades (3) discussed in the indictment. The expression of concern claims on her PLOS article says one of the fecal samples was from a dog (1) . It continues with concerns from a member of the editorial board as she said “[the article] does not provide a basis to define clinically relevant relative levels of target microbial taxa and provides minimal data on the use of 16S sequencing for clinical diagnosis.” Customers were paying with insurance based on this research and the standards were not strong enough to eliminate a sample of another species. The editorial board members comment indicates that she agrees with the indictment and does not believe it provided evidence that SmartGut is a clinical test. After the FBI raided uBiome and Bik left uBiome, @microbiomdigest was interviewed by the WSJ. In her interview with the WSJ (4), she said "The company was overselling a lot of the products." To me, this means she and others may know more about what was going with the fraudulent activity than the FBI knows. Bik continued and said "I really think that the technical part of the kit, all kits that we were selling was really good. We really had a product. We had a good product. But yeah, the interpretation of it was the issue." She knew about all of this but did not appear to report the issues to the authorities. It appears, the insurance companies made complaints that caused the FBI to investigate. She claims she "left because the company valued value over science." But she published a correction and two additional papers with the cofounders after she left the company in December of 2019. She submitted these articles before she left, but there are always some rounds of edits after submission. Before publication all authors need to do a final copywrite sign-off before publication. She had plenty of chances to prevent publishing with the indicted cofounders. Does that make any sense at all? Did she receive some sort of severance arrangement in a layoff that occurred in January 2019 (5) and that is why she finished the articles? I am confused why someone that says they left on moral grounds would continue to publish for them after she left. The last article she published with the founders and uBiome was after the FBI raided the office in April of 2019. In the WSJ interview, Amy Dockser Marcus also said " Some scientists who worked inside the company were also having reservations about what uBiome said its tests could do, like Elizabeth Bik." In the WSJ article, the author said Elisabeth helped develop SmartJane (a product heavily referenced in the indictment of not being a clinical tests and relying on the captive network of doctors to force though insurance claims). In the interview Bik said "But I felt that the vaginal microbiome would be a much better idea for clinical tests" Elisabeth Bik was involved in creating SmartJane. She knew the company was over selling. She wrote research papers that promoted the effectiveness of SmartGut (expression of concern and correction issued), SmartJane, and the reliability of upgrades. These papers were heavily referenced in the blog, press releases and marketing materials. All to say, yes, I think her past at uBiome is directly relevant to her lack of qualification to hold the title "science integrity consultant" All of these components of product, marketing, and selling came together to make the fraud work at uBiome. (1) https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0276752 (2) https://www.justice.gov/d9/press-releases/attachments/2021/03/18/ubiome_indictment_0.pdf (3) (4) https://www.wsj.com/podcasts/the-journal/what-went-wrong-at-ubiome-part-1/8b0717aa-1c66-4524-b47f-0cd3a399fcae (5) web.archive.org/web/2019100207…





@DrBMcDH - Betsy McDonel Herr, Ph.D.
Can you explain this more Dr. Hazan? I actually took the Ubiome test and it was extremely helpful. After rounds of antibiotics, showed my bif was low and Akkermansia. Metformin helps with the latter, over time other pre and probiotics for the bif. All this important for feeling well and normalizing weight.
@SabinehazanMD - sabine hazan md
ON the ubiome test… The test was not validated, compared you to mice poop, and worse the company triple billed Medicare... The fact that you got better could have just been the hand of God… In medicine, we call that the placebo effect... Believe me when I say there is a placebo effect that heals too… Having done over 300 clinical trials, I witnessed it a lot…Power of the mind… Power of God... I don't know, but the reason most drugs fail to get to market is because of the placebo effect…. After 30 years of doing clinical trials for pharma, I may know my 💩…😜
@SabinehazanMD - sabine hazan md
This tik tok had close to $1 million views last night and over 25k retweets and, in 24 hours, was pulled down @JanJekielek Do we still believe this is about a virus? They who want to control don’t want you to make discoveries. I tried to repost it, and it says “ under review” … UNDER review by WHO? I am leading the Microbiome Research clinically. Who else knows what Blautia or Roseburia does or what they are, or is it normal to have them? Please teach me... Here’s my advice; EDUCATE YOURSELF to stay alive. This is NOT about health… If it was... “discovering the loss of Bifidobacteria in severe covid patients would have hit mainstream media.” They would have pushed vitamins, exercise, and gut health for you to survive Covid. This is about control. This is about removing your freedom to speak and freedom to choose. Unite to fight for the truth. Stop the division. Your politician will not save you. @Progenabiome was created to empower you, to #letdrsbedrs, to #Savethebif. This is my life’s mission NOW!! The moment they interfered with my research, they woke me up, and I am a hurricane in research. #WATCHME #ROAR.. No Dr will innovate if this continues... No Dr will try a drug or a treatment if medicine continues to be political. We cannot afford to interfere with research because we all will be patients. Research needs to be pure and unbiased and we MUST be able to challenge the narrative.

@SabinehazanMD - sabine hazan md
Watch my post HongKong study just validated my data in a round about way…


