reSee.it - Related Post Feed

@_aussie17 - aussie17
1. New 🧵 Have you ever wondered why MOST doctors walk along the same lines when it comes to #MRNA shots, and VERY FEW doctors speak out against the narrative??? Read this thread to understand HOW Big Pharma GAGS your friendly doctor. https://t.co/nwp3ivGsC5

@_aussie17 - aussie17
2. First, you need to understand “Clinical Practice Guidelines” (lets call it “CPG”). What’s that? Officially, CPGs are guidelines that doctors refer to when treating a disease. There are guidelines for EVERY disease from Hypertension, diabetes, flu etc etc. Example 👇 https://t.co/GSBOHRkM31

@_aussie17 - aussie17
3. Within these documents, usually there is a section where they provide “Drug Choices”. They will recommend the drugs according to certain algorithms (like, whats the age of the patient, are they obese, do they have prior medical history etc etc). https://t.co/hdn8Byf5Yb


@_aussie17 - aussie17
4. In the end, it can look like a flowchart that looks like this. We call them Drug Treatment Flowcharts. https://t.co/BKvOzeaGhX

@_aussie17 - aussie17
5. Now here is what we do in Pharma. In my previous thread, I explained how we influence doctors through our Medical Sales Reps. If you haven’t read it, here is the thread.
@_aussie17 - aussie17
6. However, influencing Clinical Guidelines is another tactic altogether and it is managed by very specialized Pharma folks who usually gets paid 3 or 4 times MORE than a typical Pharma Sales Rep. Their job is to identify the committee of experts who influences these guidelines.
@_aussie17 - aussie17
7. In some countries, the experts committee who writes GUIDELINES are a secret group of doctors from their respective specialization (i.e. for Hypertension and heart diseases, a combination of cardiologists, select GPs, academias etc)
@_aussie17 - aussie17
8. Sometimes, to identify who these experts are, we employ private investigation agencies. They will find out stuffs like how frequent these committees meet, where they meet, when are the next meetings, frequency of meeting, member rotations etc.
@_aussie17 - aussie17
9. In some countries, its totally open and transparent who they are. It is complex but you get the gist. Anyway, once we identify these doctors, we INFLUENCE them through “various” means to ensure our DRUG lands as high as possible in the “Drug Choice” section of the Guidelines.
@_aussie17 - aussie17
10. Once our drug lands in the right place, the sales of those drug typically SKYROCKETS by about a factor of 5x, 10x or more. The reason is because the system is set up in a way that there is a punitive damage for doctors who do not follow the guidelines without proper reason.
@_aussie17 - aussie17
11. For example, if a doctor sees a patient with high blood pressure, he will immediately prescribe some antihypertensive drugs because of the HOLY GUIDELINES.
@_aussie17 - aussie17
12. The reason is, if a doctor recommends something like “Hey why dont you try fasting and lose some weight first?” (Which is a better treatment algorithm… but outside of GUIDELINES) if something happens to the patient after visiting the doctor (heart attack, death)…
@_aussie17 - aussie17
13….it is possible for the doctor to lose his medical license because the Medical Board will demand an explanation why they did not follow the GUIDELINES. In the end, they are forced to follow the guidelines even if they disagree, and they are not allowed to explore alternatives
@_aussie17 - aussie17
14. This is the reason why you will never hear a doctor endorse or discuss openly on alternatives (even if they are quite knowledgeable about it). They RISK losing their license, and they also risk litigations by unscrupulous patients who take advantage of these situations.
@_aussie17 - aussie17
15. That is why their response when you ask about ALTERNATIVE TREATMENTS are usually worded carefully like the CLIP from one of my favourite TV series below 😆 https://t.co/BZ34UjvOdy
@_aussie17 - aussie17
16. Now if you apply this whole situation with the #MRNA, this is exactly why many doctors are following “CDC GUIDELINES” from Mr. Fauci because they are afraid of losing their license and litigations. https://t.co/u0DXA79xgZ

@_aussie17 - aussie17
17. Fauci isn’t alone, there are many in the US who influences the FDA guidelines. Many of them have been “influenced” by Pharma and many really believe in the #clotshot. For example the doctor 👇 I will explain in other threads how we brainwash them. https://t.co/FxMw6Q2aiq
@_aussie17 - aussie17
17. We believe many have been brainwashed and they do not really know what they are recommending, but FAUCI himself we believe is a separate evil entity altogether because we think he KNOWS. Hence we wait for more revelation from @elonmusk from the coming days #TwitterFiles5
@_aussie17 - aussie17
18. There are many good ALTERNATIVE treatments for various diseases, unfortunately these treatments do not land in the GUIDELINES because of influence from the Pharma Industry. For example you will NEVER find keto/fasting which almost CURES DIABETES. Many know, but few speak up
@_aussie17 - aussie17
19. Anyway this is one of the core reasons why in the last 3 years, people have been wearing MASKS and maintaining 6 feet distancing and taking multiple #clotshots, simply because Fauci put them in the Covid Guidelines.
@_aussie17 - aussie17
20. If you enjoy this thread, please don’t forget to read my MEGA Pharma Reveal thread here.
@_aussie17 - aussie17
Many of our pharma colleagues who met Fauci said the same 👇

@goddeketal - Dr. Simon Goddek
1/ 𝗧𝗛𝗥𝗘𝗔𝗗: My name is Dr. Simon Goddek, I am a biotechnologist, and only recently @elonmusk reinstated my account after being permabanned for 1.5 years. In 2021, I took Twitter to court and curiously lost the lawsuit. #FollowTheSilenced This is my story.

@goddeketal - Dr. Simon Goddek
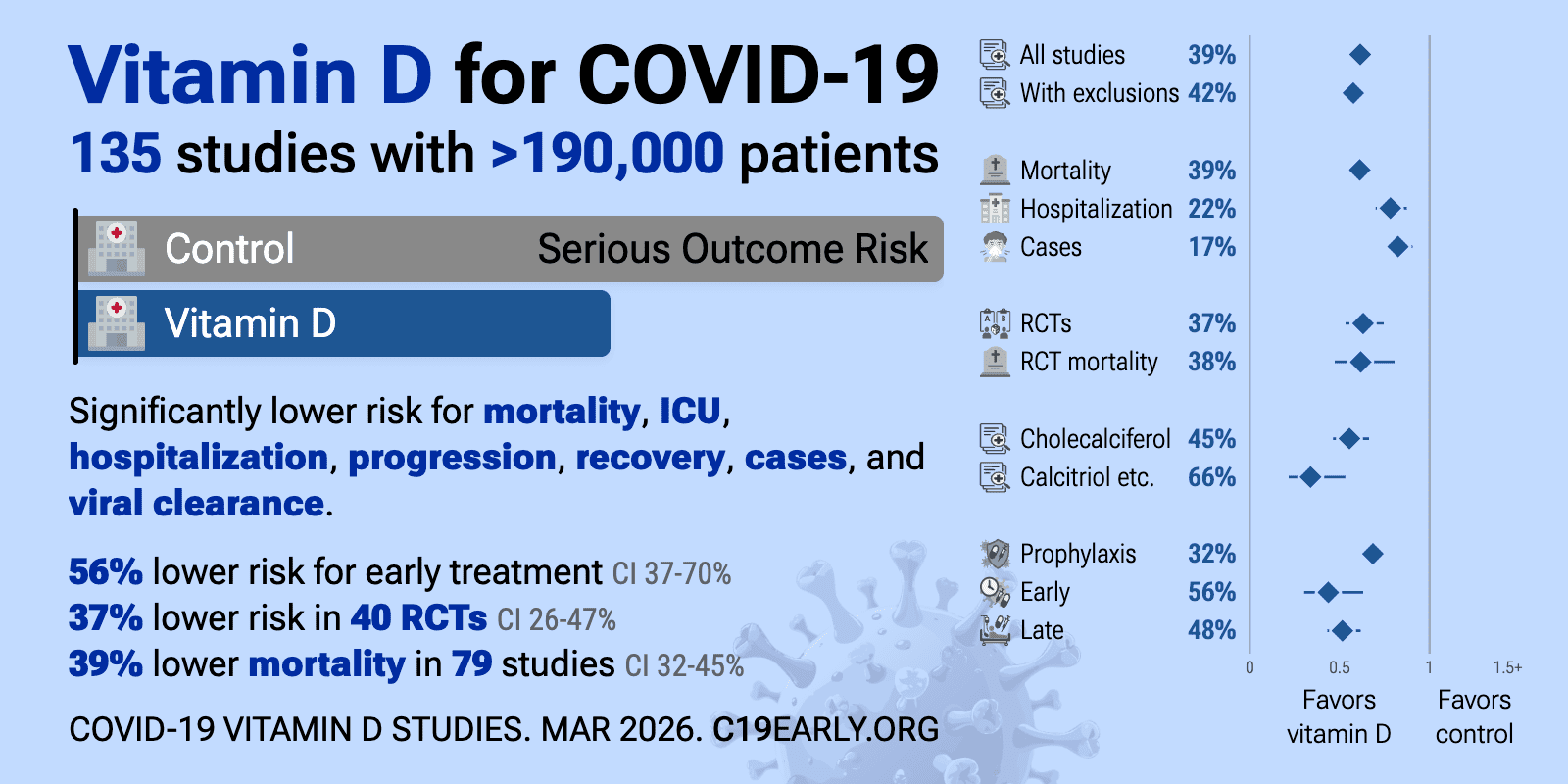
2/ While I was still cautious at the beginning of 2020 because of the pictures in Bergamo, I had wondered more and more why people were forced to wear masks and no "expert" was talking about vitamin D.

@goddeketal - Dr. Simon Goddek
3/ In good faith with science, I wrote a scientific paper on vitamin D in mid-2020 to demonstrate (by illustrating metabolic pathways) that giving "high doses" could treat covid and other health-related problems. https://pubmed.ncbi.nlm.nih.gov/32768697/

@goddeketal - Dr. Simon Goddek
4/ It didn't take long for my former employer @wur to receive the first emails. They stated that I was a pseudoscientist and corona denier. My "unscientific publication" had to be retracted immediately, was the demand of these people, who were members of the "skeptical movement".

@goddeketal - Dr. Simon Goddek
5/ I consequently became active on @twitter end of 2020. I had never been a social media person but I felt that I could no longer be silent, given the fact that I was working at a Dutch university and being an editor of a Q1 journal at that time. This is when it all started...
@goddeketal - Dr. Simon Goddek
6/ Via @waukema, I learned that the German State Virologist and fearmonger, @c_drosten, got his publication on the Covid PCR test through peer review at record time. Without this specific PCR test, we would probably never have noticed this "coronavirus".
@goddeketal - Dr. Simon Goddek
7/ I started to analyse what happened and came to the conclusion that the peer-review process was rigged as the chronology of the events shows. I consequently wrote my first Twitter thread that went viral.

@goddeketal - Dr. Simon Goddek
8/ These are the questions I raised: ▶︎ How did Drosten's paper make it through the peer review process within 24h? ▶︎ How does he even publish there while being part of the journal's editorial board? ▶︎ Why does the journal refuse to publish anonymous peer-review reports?
@goddeketal - Dr. Simon Goddek
9/ Overnight I gained thousands of followers and was heavily attacked by virologists from @UniUtrecht and @erasmusuni. They tried everything to get me to take my thread (see substack link) offline. This was my first contact with the cancel culture movement.https://drsimon.substack.com/publish/post/74797608
@goddeketal - Dr. Simon Goddek
10/ I did some more digging and also learned that @c_drosten… ▶︎ Created that specific PCR test most likely even before the outbreak of the pandemic ▶︎ Denied viral seasonality (https://t.me/goddek/1295) ▶︎ Made contradictory statements about masks (https://t.me/goddek/563)


@goddeketal - Dr. Simon Goddek
11/ …and… ▶︎ Predicted piles of corpses on African streets (https://bit.ly/3ictjy4) ▶︎ Called renowned dissidents "pseudoscientists" (https://bit.ly/36ngzle) ▶︎ Got funds from the @gatesfoundation and had his professorship sponsored by Nazi-money (Quandt Family)


@goddeketal - Dr. Simon Goddek
12/ Questions upon questions and still no answers. My account grew. I began to post more studies, for example, about the efficacy of masks, the implementation of arbitrary measures and their effects on public health, the potential of vitamin D, etc.
@goddeketal - Dr. Simon Goddek
13/ The more I wrote, the more "fan mail" my then-employer @wur got. My research funding expired in March 2021, but I had written an EU-funding proposal in 2020 (in my spare time) to prolong my employment. The chance to win was 1% and guess what - I won. 🥳
@goddeketal - Dr. Simon Goddek
14/ Even though @wur backed me and I personally raised a large amount of funding for them, I was told by phone that I would be dismissed from my position because of my tweets. They would use the money I generated to hire someone less critical. Overnight, I was out of a job.

@goddeketal - Dr. Simon Goddek
15/ Since life in 🇳🇱 was too expensive for an unemployed person, I decided to move to 🇧🇷 to live with my partner. There I bought a few hectares of land in the jungle to escape the madness. I had to leave my family and friends behind. It hurt, but I did not have much of a choice.

@goddeketal - Dr. Simon Goddek
16/ These were difficult months for me. The feeling of being treated unfairly and cancelled was suffocating. I just couldn't sit on it. I decided to take Twitter to court. "Justice will prevail", I thought. A naive thought, as it would later turn out.
@goddeketal - Dr. Simon Goddek
17/ My posts must have consistently been a thorn in the side of the woke fact-checkers from Twitter's Ministry of Truth, and I've regularly been temporarily banned from Twitter for statements that are mainstream these days. Here are a few examples. #cringealert

@goddeketal - Dr. Simon Goddek
18/ 𝗘𝗫𝗔𝗠𝗣𝗟𝗘 𝗢𝗡𝗘: I referred to this publication (https://www.mdpi.com/1660-4601/18/8/4344), which has been peer-reviewed. Twitter banned me for doing so for one week for "Violating the policy on spreading misleading and potentially harmful information related to COVID-19.".

@goddeketal - Dr. Simon Goddek
19/ 𝗘𝗫𝗔𝗠𝗣𝗟𝗘 𝗧𝗪𝗢: I cited (!!!) a scientist from an official Texas Senate hearing and posted the corresponding video. See:

@goddeketal - Dr. Simon Goddek
20/ 𝗘𝗫𝗔𝗠𝗣𝗟𝗘 𝗧𝗛𝗥𝗘𝗘: Here, I referred to meta-analyses that are available on http://vdmeta.com and http://c19ivm.org. Fun fact: the scientists that are running these websites have been banned from @twitter, too.


@goddeketal - Dr. Simon Goddek
21/ 𝗘𝗫𝗔𝗠𝗣𝗟𝗘 𝗙𝗢𝗨𝗥: In June 2021, I was banned for asking questions. The @gatesfoundation really invested that much into BioNTech (https://endpts.com/biontech-partners-with-bill-and-melinda-gates-foundation-scoring-55m-equity-investment-novartis-sells-china-unit/). Why was it prohibited to ask questions?


@goddeketal - Dr. Simon Goddek
22/ One day later, my account got permabanned. My impact was probably too big (400 new followers per day and 3K likes on average) that Twitter pulled the ripcord. My account was banned for "targeted harassment" without Twitter providing me with a specific explanation.

@goddeketal - Dr. Simon Goddek
23/ Even after requesting further information about permanently locking my account, Twitter refused to give me the actual or specific reason for the suspension. Since I had moved to Brazil in the meantime, I took Twitter to court here.
@goddeketal - Dr. Simon Goddek
24/ I contracted one of the best lawyers for media law in Brazil, who informed me in beforehand that Twitter is the worst social medium and that they usually do not care about free speech. He told me that there is a high likelihood that they’d have to reinstate my account.
@goddeketal - Dr. Simon Goddek
25/ However, due to the "pandemic," the hearing could not take place in person. Instead, we had a Zoom Call. Present were the judge, my lawyer, me and six (!!!) lawyers for Twitter.
@goddeketal - Dr. Simon Goddek
26/ The Brazilian armada of Twitter lawyers explained during the trial that I was not banned for "targeted harassment" but for spreading dangerous medical falsehoods (i.e. Twitter initially lied). Nevertheless, I was also presented with the tweet that led to my final suspension.

@goddeketal - Dr. Simon Goddek
27/ The second hearing was in writing only. The judge's decision was then made in March 2022. It was argued that it did not matter whether my statements were correct or not. According to the judge, Twitter has digital domiciliary rights in Brazil.
@goddeketal - Dr. Simon Goddek
28/ The Twitter chapter was therefore closed for me. My permaban was politically motivated and there was nothing I could do about it. So I put my energy into my Telegram channel (https://t.me/goddek) and my new permacultural life in the Brazilian wilderness.

@goddeketal - Dr. Simon Goddek
29/ In the meantime I have found a new job and my Twitter account has been reinstated thanks to @elonmusk. What remains is that we have been insulted, cancelled, ridiculed, and publicly discredited for speaking out against irrational measures.
@goddeketal - Dr. Simon Goddek
@elonmusk 30/ My story is one of millions. Many of you have surely suffered a similar, if not worse, fate. That is precisely why we must stick together and support each other. My PMs are open and on @telegram I read every single one of your comments. It's wonderful that you all exist!
@goddeketal - Dr. Simon Goddek
@elonmusk @telegram 31/ We who have been cancelled must finally be heard again. Hence #FollowTheSilenced instead of #FollowTheScience. My story was just one of many. Many like-minded people share a similar fate with me. Some of them are...
@goddeketal - Dr. Simon Goddek
@elonmusk @telegram 32/ Journalists such as: @naomirwolf, @tracybeanz, @vigilantfox, @thechiefnerd, @KanekoaTheGreat, @kylenabecker, @ElectionWiz, @RealJermWarfare, @ChelleWards, @usmortality, @MichaelPSenger, @jeffreyatucker, @danastingregory, @YaffaRaz, @jamesfWells, @EtanaHechtDC...
@goddeketal - Dr. Simon Goddek
33/ @delbigtree, @hodgetwins, @ShellenbergerMD, @MarioNawfal, @Lukewearechange, @SebGorka, @greggutfeld, @EmeraldRobinson, @sonia_elijah, @beverleyturner, @chrismartenson, @JanJekielek, @mrmarkdolan, @ianmSC, @EthicalSkeptic, @birb_k, @JordanSchachtel.
@goddeketal - Dr. Simon Goddek
@delbigtree @hodgetwins @ShellenbergerMD @MarioNawfal @Lukewearechange @SebGorka @greggutfeld @EmeraldRobinson @sonia_elijah @beverleyturner @chrismartenson @JanJekielek @mrmarkdolan @ianmSC @EthicalSkeptic @birb_k @JordanSchachtel 34/ Freedom activists such as: @TexasLindsay_, @robinmonotti, @liz_churchill8, @DSchlopesIsBack, @DowdEdward, @Lilith_Assyria, @Large_Farm, @bobscartoons, @stkirsch, @thecoastguy, @efenigson, @RobertKennedyJR, @prof_freedom, @TaraBull808, @FiveTimesAugust, @BrendanEich, @ooana.
@goddeketal - Dr. Simon Goddek
@delbigtree @hodgetwins @ShellenbergerMD @MarioNawfal @Lukewearechange @SebGorka @greggutfeld @EmeraldRobinson @sonia_elijah @beverleyturner @chrismartenson @JanJekielek @mrmarkdolan @ianmSC @EthicalSkeptic @birb_k @JordanSchachtel @TexasLindsay_ @robinmonotti @liz_churchill8 @DschlopesIsBack @DowdEdward @Lilith_Assyria @Large_Farm @bobscartoons @stkirsch @thecoastguy @efenigson @RobertKennedyJr @prof_freedom @TaraBull808 @FiveTimesAugust @BrendanEich @ooana 35/ Scientists such as: @JesslovesMJK, @RWMaloneMD, @drmikehart, @DrLoupis, @molsjames, @MarkChangizi, @DrEliDavid, @DrJBhattacharya, @UngaTheGreat, @RealJoelSmalley, @davidjthunder, @FatEmperor, @Mala_Naicker, @jordanbpeterson.
@goddeketal - Dr. Simon Goddek
@delbigtree @hodgetwins @ShellenbergerMD @MarioNawfal @Lukewearechange @SebGorka @greggutfeld @EmeraldRobinson @sonia_elijah @beverleyturner @chrismartenson @JanJekielek @mrmarkdolan @ianmSC @EthicalSkeptic @birb_k @JordanSchachtel @TexasLindsay_ @robinmonotti @liz_churchill8 @DschlopesIsBack @DowdEdward @Lilith_Assyria @Large_Farm @bobscartoons @stkirsch @thecoastguy @efenigson @RobertKennedyJr @prof_freedom @TaraBull808 @FiveTimesAugust @BrendanEich @ooana @JesslovesMJK @RWMaloneMD @drmikehart 36/ @MartinKulldorff, @MartyMakary, @zoeharcombe, @DrPPhillipsMD, @MLevitt_NP2013, @SHomburg, @NaturallyFTW, @jikkyleaks, @IamBrookJackson, @denisrancourt, @PoliticalMoons2, @MikeDonio, @goddeketal (me).
@goddeketal - Dr. Simon Goddek
@delbigtree @hodgetwins @ShellenbergerMD @MarioNawfal @Lukewearechange @SebGorka @greggutfeld @EmeraldRobinson @sonia_elijah @beverleyturner @chrismartenson @JanJekielek @mrmarkdolan @ianmSC @EthicalSkeptic @birb_k @JordanSchachtel @TexasLindsay_ @robinmonotti @liz_churchill8 @DschlopesIsBack @DowdEdward @Lilith_Assyria @Large_Farm @bobscartoons @stkirsch @thecoastguy @efenigson @RobertKennedyJr @prof_freedom @TaraBull808 @FiveTimesAugust @BrendanEich @ooana @JesslovesMJK @RWMaloneMD @drmikehart 37/ MDs such as: @doc_singing, @KLVeritas, @DrTeckKhong, @MdBreathe, @LynnFynn3, @Doctor_Iver, @drcole12, @richardursomd, @DrJackieStone, @SabinehazanMD, @NeputeWellness, @lawrie_dr, @P_McCulloughMD.
@goddeketal - Dr. Simon Goddek
@delbigtree @hodgetwins @ShellenbergerMD @MarioNawfal @Lukewearechange @SebGorka @greggutfeld @EmeraldRobinson @sonia_elijah @beverleyturner @chrismartenson @JanJekielek @mrmarkdolan @ianmSC @EthicalSkeptic @birb_k @JordanSchachtel @TexasLindsay_ @robinmonotti @liz_churchill8 @DschlopesIsBack @DowdEdward @Lilith_Assyria @Large_Farm @bobscartoons @stkirsch @thecoastguy @efenigson @RobertKennedyJr @prof_freedom @TaraBull808 @FiveTimesAugust @BrendanEich @ooana @JesslovesMJK 38/ @Doctor_I_am_The, @Saikmedi, @houmanhemmati, @Tom_Rumi, @arkmedic, @BrianLenzkes, @kacdnp91, @molsjames, @dockaurG, @DrKellyVictory, @akheriaty, @DrHenryEaly, @PierreKory, @GeorgeFareed2, @DrSyedHaider.
@goddeketal - Dr. Simon Goddek
@delbigtree @hodgetwins @ShellenbergerMD @MarioNawfal @Lukewearechange @SebGorka @greggutfeld @EmeraldRobinson @sonia_elijah @beverleyturner @chrismartenson @JanJekielek @mrmarkdolan @ianmSC @EthicalSkeptic @birb_k @JordanSchachtel @TexasLindsay_ @robinmonotti @liz_churchill8 @DschlopesIsBack @DowdEdward @Lilith_Assyria @Large_Farm @bobscartoons @stkirsch @thecoastguy @efenigson @RobertKennedyJr @prof_freedom @TaraBull808 @FiveTimesAugust @BrendanEich @ooana @JesslovesMJK @Doctor_I_am_The @Saikmedi @houmanhemmati @Tom_Rumi @arkmedic @BrianLenzkes @kacdnp91 @molsjames 39/ Politicians such as: @ABridgen, @RickNichollsCKL, @mrddmia, @RepTroyNehls, @BrianKempGA, @repmattgaetz, @ChrisLandauUSA.
@goddeketal - Dr. Simon Goddek
@delbigtree @hodgetwins @ShellenbergerMD @MarioNawfal @Lukewearechange @SebGorka @greggutfeld @EmeraldRobinson @sonia_elijah @beverleyturner @chrismartenson @JanJekielek @mrmarkdolan @ianmSC @EthicalSkeptic @birb_k @JordanSchachtel @TexasLindsay_ @robinmonotti @liz_churchill8 @DschlopesIsBack @DowdEdward @Lilith_Assyria @Large_Farm @bobscartoons @stkirsch @thecoastguy @efenigson @RobertKennedyJr @prof_freedom @TaraBull808 @FiveTimesAugust @BrendanEich @ooana @JesslovesMJK @Doctor_I_am_The @Saikmedi @houmanhemmati @Tom_Rumi @arkmedic @BrianLenzkes @kacdnp91 @molsjames @ABridgen @RickNichollsCKL @mrddmia @RepTroyNehls @BrianKempGA @RepMattGaetz 40/ Many of them will also share their personal stories over the next few days under the hashtag #FollowTheSilenced. Please follow them so that they may never be silenced again. Cheers and thanks for joining the fight for freedom. Simon (@goddeketal)

@TheOriginalSai - Sai
1. Thread: THE TRUTH ABOUT THE COVID-19 PANDEMIC FROM WITHIN THE NHS (EX DIRECTOR OF END OF LIFE CARE AT ONE OF THE LARGEST HOSPITAL TRUSTS IN THE UK) #NHS #Truth #Awareness #World #Freedom #Humanity #PowerToThePeople #Healthcare #COVID19 #CovidVaccine #VaccineDeath #Pandemic
@TheOriginalSai - Sai
2. In 2016, the British Government proposed & piloted a change to the process of how deaths were certified across all hospitals in the UK. I have attached a link to this Department of Health (DoH) document below: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/521226/Death_certificate_reforms_pilots_-_report_A.pdf
@TheOriginalSai - Sai
3. The DoH document proposed a switch to the "Medical Examiner" (ME) System and was sent to a number of different audiences for feedback and consultation. The ME system was already being piloted at two hospitals up north. The results of the consultation are below:
@TheOriginalSai - Sai
@TheOriginalSai - Sai
5. Prior to the Covid-19 Pandemic, the death certification process involved treating doctors of a patient to attend Bereavement Services/Patient Affairs to discuss the death and either: a) refer the death to the Coroner or b) write a Medical Certificate of Cause of Death (MCCD)
@TheOriginalSai - Sai
6. The MCCD states the cause of death. Whereby a direct cause (1a) or contributing causes (1b) (1c) (1d) are stated along with co-morbidities (not directly causing the death) being written in (2) on the MCCD. The MCCD is only ever a probable cause of death, it is not definitive.
@TheOriginalSai - Sai
7. The only definitive way of determining an accurate and plausible cause of death is to refer the deceased patient to HM Coroner (if certain criteria is met), for HM Coroner to accept and take on the case, resulting in a Post Mortem (PM) being conducted by a Histopathologist.
@TheOriginalSai - Sai
8. When a death is seen as natural and there is nothing untoward, the MCCD is written by the treating doctor of a deceased patient. Usually this is an F1, F2, SHO or Registrar that attends. It is rare for a treating Consultant to attend, but they will finalise the cause of death.
@TheOriginalSai - Sai
9. A strict hospital hierarchy exists within the NHS for doctors. It is as follows - from lowest to highest rank: Foundation Year 1 (FY1), Foundation Year 2 (FY2), Senior House Officer (SHO), Registrar (Reg), Consultant, Clinical Lead, Medical Director.
@TheOriginalSai - Sai
10. Junior doctors will very rarely speak up or challenge their seniors. A senior decision is seen as final and it will be carried out and executed without any hesitance or questioning.
@TheOriginalSai - Sai
11. In my 5.5 years of experience in End of Life Care, I have only ever seen one junior doctor disagree with a proposed cause of death and challenge their consultant.
@TheOriginalSai - Sai
12. With the number of deaths that occur in a hospital, as you can imagine, there is a great deal of variation with regards to causes of death, as we have numerous different doctors writing an MCCD and coming up with various different potential diseases in different orders.
@TheOriginalSai - Sai
13. The proposed ME system would change this, as the government would now hire and pay one Medical Examiner, to sit in every hospital and write all MCCD's for all deceased patients. This would effectively eliminate any variation in causes of death.
@TheOriginalSai - Sai
14. In 2016, when I heard of this proposal, I worked as a Bereavement Officer at a hospital in Central London. My mentor/line manager at the time was a former Chief Nurse who managed Bereavement Services and all hospital deaths would be controlled by her and the department.
@TheOriginalSai - Sai
15. We essentially carried a huge amount of power with regards to decision making, as we would go through all patient notes following the death of a patient, and essentially guide and advise doctors on what would need to be written with regards to an MCCD or Coroners Referral.
@TheOriginalSai - Sai
16. In my personal opinion, our role was to sit on the fence and act in the best interests of a deceased patient (and their families), but also protect the hospital and our doctors from any potential negligence.
@TheOriginalSai - Sai
17. As you can imagine many battles were fought over decisions about a cause of death of a patient or a referral to the coroner with a vast amount of doctors over the years.
@TheOriginalSai - Sai
18. F2's and SHO's were particularly the worst with regards to carrying an arrogance of knowing what should be written on an MCCD or stating that a patient didn't need to be referred to the Coroner (often stating that their Consultant had given them instructions).
@TheOriginalSai - Sai
19. It is worth noting that Consultants are also only human and can be incorrect at times too. We have to remember that they are succeeded in hierarchy by a Clinical Lead and beyond that a Medical Director. Who have far more experience and knowledge.
@TheOriginalSai - Sai
20. When I asked my mentor in 2016, how the ME system would change things, I was told that Bereavement Services/Patient Affairs would become purely administrative and that the clinical judgement would fall to the Medical Examiner.
@TheOriginalSai - Sai
21. The power and decision making with regards to MCCD/Coroners Referrals was being taken away not only from treating doctors but also from Bereavement Services/Patient Affairs/Bereavement Officers/Bereavement Service Managers/Directors of End of Life Care.
@TheOriginalSai - Sai
22. This decision making power was being handed solely to the Medical Examiner, who has not been involved in the treatment of a patient during an admission. I took all this information in at the time and acquired as much knowledge as I could from my mentor/line manager.
@TheOriginalSai - Sai
23. In 2016, I also happened to make a move and take up an opportunity to manage my own Bereavement Services at one of the largest hospital trusts in the whole of the UK. On average, I would oversee MCCD/Coroner Referrals for approx 1750 deaths on an annual basis.
@TheOriginalSai - Sai
24. I developed a very close working relationship and friendship with one of the Medical Directors (a doctor with the highest ranking in a hospital). This was especially helpful when having to challenge doctors with regards to MCCDs/Coroners Referrals.
@TheOriginalSai - Sai
25. Progressing to Director of End of Life Care, I became involved with the reporting of mortality rates, conducting mortality reviews and writing hospital policies. I had also developed an excellent working relationship with the HM Coroner who oversaw our Trust. TBC...
@TheOriginalSai - Sai
26. HM Coroner holds the power to investigate any hospital or trust with regards to a death or a number of deaths. A slight problem may arise, in that HM Coroner has an allegiance to the Crown and the Government.
@TheOriginalSai - Sai
27. When a death is reported to the Coroner. This was previously reported via telephone call by the treating doctor. A discussion was had with the Coroners Office and an direct outcome and instruction would come from the Coroner's Office, by way of HM Coroner (via a phonecall).
@TheOriginalSai - Sai
28. There is a fundamental flaw to this system, as there is no documentation of the decision and instruction from the Coroner's. It comes via word of mouth. There is always room for error without any electronic documentation.
@TheOriginalSai - Sai
29. Every Hospital/Trust & HM Coroner will have a different system of reporting deaths. I personally made a decision to safeguard my hospital and the trust, by developing an electronic coroners referral form, which I proposed to our Coroner and developed after their agreement.
@TheOriginalSai - Sai
30. We now had documentation of every death being reported and every outcome. When reporting a death, the Coroner will look at a proposed cause of death and accept it, or reject the cause of death and take on the case (death of the patient), leading to an Inquest or a PM.
@TheOriginalSai - Sai
31. In 2019, our Medical Director, came into my office one morning and stated that the Board of Directors at the Hospital had made a decision to switch to the Medical Examiner System. Hearing the words ME system was a massive case of Déjà vu (conversation with my mentor in 2016)
@TheOriginalSai - Sai
32. I knew exactly what the ME system was, but I chose instead, to play the fool and enquire what exactly the ME system was and what it meant for our service, my staff and our roles. Everything the Medical Director mentioned to me that day was a carbon copy of what I already knew
@TheOriginalSai - Sai
33. I knew that my time in End of Life Care had come to an end. I'd reached the top and there was no more progress for me. Losing all power and decision making to any ME coming into the hospital did not appeal to me. I'd already made up my mind that I needed to leave.
@TheOriginalSai - Sai
34. Seeking a new challenge and experience, I made a move in 2019 to another major hospital in Central London, this time sidetracking into operational management. I was in charge of the operational management of Nephrology, Rheumatology, Dermatology and Diabetes & Endocrinology.
@TheOriginalSai - Sai
35. In Jan 2020, I remember hearing about the first case of Covid-19 at our hospital, with a patient arriving from China and walking into our A&E. A&E was shutdown and steam cleaned that day, I recollect the moment I heard about this.
@TheOriginalSai - Sai
36. In my mind, I saw the reporting of Covid-19 in the media as nothing more than Bird Flu or Ebola, which had caused panic but yet passed. I wasn't worried in the slightest bit. Things began to escalate around in Feb 2020, around the time I was going on holiday.
@TheOriginalSai - Sai
37. Due to the reporting by the media, I bought N95 masks as a precaution for my trip and to give to my parents and younger sister. I was blessed to have had an opportunity to spend a few days in Sri Lanka for a wedding and then nearly a whole month in Australia (March 2020).
@TheOriginalSai - Sai
38. I watched as the narrative of a deadly infectious disease continued to grow with every day that passed. I made a decision to cut my holiday short by a couple of days so that I could make sure I got back to my family and not end up being stranded in Australia.
@TheOriginalSai - Sai
39. Upon returning to the UK in late March 2020. One of the immediate things that struck me was the lack of any temperature monitoring or questioning at Heathrow Airport. This seemed odd for a potentially deadly infectious disease that was spreading around the world.
@TheOriginalSai - Sai
40. This was especially odd, as Sri Lanka & Australia had questioned me/checked temperatures upon arrival, with even Singapore monitoring temperatures during transit.
@TheOriginalSai - Sai
41. My mother had just recovered from Cancer, my father was over 70 and my younger sister was born with Down's Syndrome alongside having multiple other conditions. I had three high risk individuals to Covid-19 in my family and I was scared/fearful of giving them Covid-19.
@TheOriginalSai - Sai
42. I asked my hospital to allow me to work from home. They refused. I wasn't deemed high risk, although I lived with my parents at the time. I needed to help my mum and my sister. The hospital held no regard for the safety of it's employees. They forced me to come into work.
@TheOriginalSai - Sai
43. I spent two months isolating in my bedroom, I barely came out of my room, for fear of spreading an infectious disease. Never once did I think about the situation or my prior experience or knowledge, I was just reacting to the media frenzy. I was full of panic and stress.
@TheOriginalSai - Sai
44. The first irregularity I noticed, was the government and media stating that Covid-19 was an infectious disease. However just before the first lockdown was implemented, I noted that the government had downgraded the status of Covid-19 stating it was no longer infectious.
@TheOriginalSai - Sai
45. This made no sense to me. Why would we need to isolate if they downgraded the status? My circle of friends contained many medics and dentists. They were all panicking at the time, saying they had inadequate surgical masks and that they needed N95 masks.
@TheOriginalSai - Sai
46. N95 masks were seen as the only way to prevent medical professionals from becoming infected with Covid-19. The public being asked to wear surgical masks made no sense to me. The virus would be able to go straight through. Something didn't seem right.
@TheOriginalSai - Sai
47. I ended up meeting and dating an FY1 doctor (my ex gf) around October 2020. We clicked because she was different from every other doctor, I had previously spoken to about Covid-19. She also had her suspicions and believed it wasn't as infectious as it was made out to be.
@TheOriginalSai - Sai
48. We both started to slowly realise that Covid-19 was a real disease (as it was showing up on X-rays in patients) but that it wasn't infectious at all, despite all the reporting in the media.
@TheOriginalSai - Sai
49. I needed to experience working in a Covid-19 hotspot and see all the action for myself. In March 2021, I quit my job at the hospital in Central London and took up an opportunity to manage A&E and AMU (Acute Medical Unit) at a hospital in South London.
@TheOriginalSai - Sai
50. The 6 months that I spent working in A&E/AMU confirmed all my suspicions and culminated in my decision to end my career in the NHS. TBC
@TheOriginalSai - Sai
51. The entire 6 months, I was not tested once with a PCR Test, despite walking into wards full of Covid-19 Positive patients on a daily basis. Yet we were required to test multiple times when visiting another country.
@TheOriginalSai - Sai
52. The PCR Test that the NHS was using to test patients, is known to have a false-positive results. This is shown in numerous studies which can be found online, an example of which is: https://www.cebm.net/covid-19/infectious-positive-pcr-test-result-covid-19/
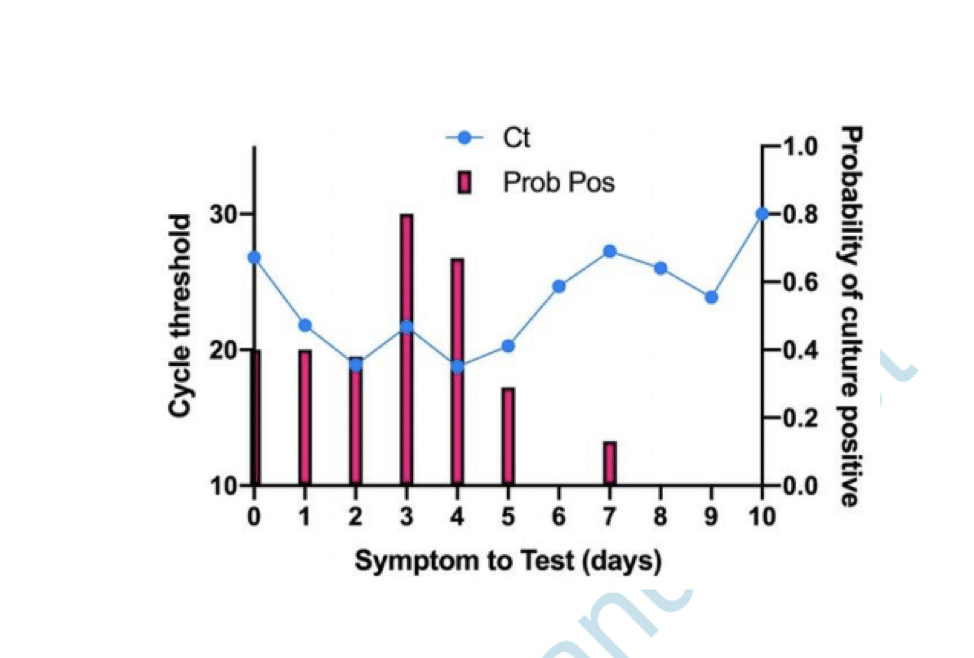
@TheOriginalSai - Sai
53. If a patient tests positive for Covid-19 with a PCR Test, this doesn't mean they are infected. If tested again, they may well turn out with a negative test. However in the NHS, patients are only tested once and this stays on their record throughout their admission.
@TheOriginalSai - Sai
54. Hospital policies were changed alongside the implementation of the Medical Examiner System, to ensure that any patient who died within 30 days of positive test, would have to have Covid-19 as their primary cause of death. This was regulated by the Medical Examiner.
@TheOriginalSai - Sai
55. The highest cause of death at every hospital per annum pre Covid-19 is Pneumonia. Pneumonia is a Respiratory Disease like Covid-19. Pneumonia can be broken down into 4 different causes of death:
@TheOriginalSai - Sai
56. Pneumonia can be broken down into 4 different causes of death: Bronchopneumonia, Aspiration Pneumonia, Community Acquired Pneumonia & Hospital Acquired Pneumonia. These four causes when added together kill the largest number of people on an annual basis prior to the pandemic
@TheOriginalSai - Sai
57. The Medical Examiner (one individual in each hospital), was certifying all these Pneumonia deaths as Covid-19 deaths. When 4 different diseases being grouped and now being called Covid-19, you will inevitably see Covid-19 with a huge death rate.
@TheOriginalSai - Sai
58. The mainstream media was reporting on this huge increase in Covid-19 deaths due to the Medical Examiner system being in place.
@TheOriginalSai - Sai
59. Patients being admitted and dying with very common conditions such as Old Age, Myocardial Infarctions, End Stage Kidney Failure, Haemorrhages, Strokes, COPD & Cancer etc were all now being certified as Covid-19 via the Medical Examiner System.
@TheOriginalSai - Sai
60. Hospitals were switching to and from the Medical Examiner system and the Pre Pandemic System as when they pleased. When Covid-19 deaths needed to be increased, the hospital would switch to the Medical Examiner System.
@TheOriginalSai - Sai
61. Doctors were one week being told they needed to complete an MCCD, to then be told the following week that they weren't required to fill out an MCCD, as the Medical Examiner was handling this.
@TheOriginalSai - Sai
62. Hospitals were incentivised to report Covid-19 deaths over normal deaths, as the government was paying hospitals additional money for every Covid-19 death that was being reported. The Medical Examiner system ensured that Covid-19 was being put down as the cause of death.
@TheOriginalSai - Sai
63. The government sends out the annual NHS budget to Primary Care Trusts. This is split to fund Hospitals and GP Surgeries. A clinical coding team at each hospital will assign codes to each treatment or death, so that money is paid out to the hospitals.
@TheOriginalSai - Sai
63. Any doctor who argued against Covid-19 as a cause of death was bullied and vilified. The General Medical Council maintains a register of all doctors within the UK. This ensures that there is a fear of being struck off for speaking out against an agenda.
@TheOriginalSai - Sai
64. The GMC effectively controls all doctors in the UK. Even if a doctor realises what is going on and wants to speak out. They will think twice about talking, as they would be risking their entire career and everything that they've worked so hard for.
@TheOriginalSai - Sai
65. Doctors essentially have their hands tied, many have families, kids, mortgages and mouths to feed. If I was in their situation, I would think twice about speaking out, for fear of being struck off by the GMC and losing everything.
@TheOriginalSai - Sai
66. The NHS Track & Trace App, which was introduced to try and control the spread of the virus, did not apply to medical professionals. We were all asked to turn this off, as Doctors and staff isolating for 14 days disrupted patient flow, beds and the discharge of patients.
@TheOriginalSai - Sai
67. Any doctor that I spoke to regarding taking the Covid-19 vaccine, were insistent that they were going to wait for a period of time, before taking it themselves, to ensure that it was safe. How is it ethical to give a vaccine to your patients, but not want to take it yourself
@TheOriginalSai - Sai
68. In my 12 years of NHS service, never has a doctor pushed or influenced the public to take a vaccine. Yet on social media, I was seeing close friends who were doctors, starting to post on social media that they have taken the vaccine and that the public should.
@TheOriginalSai - Sai
69. I wouldn't be surprised if doctors were being forced to promote the vaccine by their superiors or if they were receiving monetary gain in doing so.
@TheOriginalSai - Sai
70. I have no doubt in my mind, that the Government has planned the entire pandemic since 2016, when they first proposed the change to medical death certification.
@TheOriginalSai - Sai
71. Stress leads to disease and illness. Panic leads to people following whatever orders and instructions that are given to them by authority, such as prolonged mask use, which leads to an increase in admissions in to the NHS system due to hypoxia and bacterial pneumonia.
@TheOriginalSai - Sai
72. The NHS treatment pathway involved patients being placed onto ventilators. There is a 50% chance of death from this clinical decision alone. How many innocent people have died from the clinical decision to place them onto a ventilator. TBC
@TheOriginalSai - Sai
73. During boardrounds (where every admitted patient is discussed), we were seeing patients on a daily basis being admitted due to suffering from adverse affects of taking the vaccine. Patients were blacking out after taking the vaccine or suffering from clots or strokes.
@TheOriginalSai - Sai
74. The NHS is all about money and making money. The safety of a patient didn't seem like the most important thing. It was more about how do we make more beds available so that another patient can be treated.
@TheOriginalSai - Sai
75. Patients with no next of kin are discharged to nursing homes with care packages. I can't comment on what happened to these patients in nursing homes, during the pandemic, as I have no experience of their inner workings.
@TheOriginalSai - Sai
76. Patients are seen as money, even upon death, hospitals receive money for each death. Is there an actual concern for patient health and safety? I know numerous doctors who are driven primarily by money and monetary gain.
@TheOriginalSai - Sai
77. THE REASON WHY I LEFT THE NHS in 2021 56 yr old male, admitted into a&e with end stage kidney failure, has a previous history of regular dialysis treatment for this. No respiratory symptoms on admission and no temperature. However when tested with a PCR Test...
@TheOriginalSai - Sai
he unfortunately tests positive. This stays on his record throughout his admission. Our hospital is relatively small in comparison to others I have worked at, we have no dialysis machine as a result. We urgently need to transfer this patient to another hospital....
@TheOriginalSai - Sai
otherwise this patient will die. Our treating doctor calls up larger hospitals with a dialysis machine to organise his transfer. All doctors pick up the phone and request the Covid-19 status of the patient. A transfer is declined due to a Covid-19 infection protocol....
@TheOriginalSai - Sai
Our doctors again reiterate the point that this patient will die without dialysis. We are told there is nothing that can be done and that the patient cannot be accepted for transfer. This gentleman ended up dying without dialysis. Now please tell me what goes on the MCCD....
@TheOriginalSai - Sai
1a) Covid-19 2) End Stage Kidney Failure Not written by the treating doctor who disagreed with this cause of death, but by a medical examiner, put in place by the government and the hospital.
@TheOriginalSai - Sai
When innocent people are being killed by a corrupt organisation and system, for pure monetary gain, I can't stand by and be part of this anymore. My conscious was clear and I no longer wanted to be a part of this anymore.
@TheOriginalSai - Sai
78. I am very blessed and lucky that I was in a position to walk away. I've been able to speak out, because my hands are not tied and I am not regulated by any organisation or governing body. I believe in speaking the truth and in doing so, I am only just an instrument for God.
@TheOriginalSai - Sai
79. I joined the NHS, 12 years ago because I had a desire to help those in need, but the moment I realised that I was not doing this anymore was the time for me to walk away.
@TheOriginalSai - Sai
80. I apologise to you all if the above thread is confusing with regards to terminology or you cannot understand it's contents. I'm hoping that at the very least, it can be understood by my fellow medical professionals or by journalists who would like to report the truth.
@TheOriginalSai - Sai
81. Would be very grateful if you could help spread this truth and raise awareness of what really went on within the NHS by reposting and tagging any relevant individuals who you think may help with spreading the truth of this thread. God Bless You All ❤️

@drkohilathas - Dr. Eashwarran Kohilathas
Some of you have recently discovered me, whilst others have known me for a few years now. Many of you may be wondering where I had been and what I was doing, whilst others know me quite well. To get everyone on the same page, I thought it would be good to tell a little story.
@drkohilathas - Dr. Eashwarran Kohilathas
In late 2019 and early 2020 I was asked to work front line in an emergency department to help with the "war effort". We had no idea what was going on, apart from a few videos of the Chinese suddenly collapsing due to this new contagion. We were waiting for it to hit the UK.
@drkohilathas - Dr. Eashwarran Kohilathas
It hit, I saw what it did to people, people became unwell, xray xray xray, PPE, barriers, red lights, code words, panic panic. Our world changed overnight, and my world changed especially. One minute we were told not to wear masks, the next moment it was made mandatory etc.
@drkohilathas - Dr. Eashwarran Kohilathas
My sole focus was to protect myself and my family at this point, and so in efforts to do this successfully I began studying. I read papers during my breaks, at night, before work. I reflected on what I saw at work, and made a mental note of real life evidence.
@drkohilathas - Dr. Eashwarran Kohilathas
The emergency department warped as time went on, I saw a lot of errors happening and mismanagement of resources. Patient care was being delayed and this led to staff burnout and medical errors. I could see that if this went on, people would needlessly die.
@drkohilathas - Dr. Eashwarran Kohilathas
I knew something had to change. So in efforts to bring about some change, I wrote a book outlining how Toyota lean manufacturing methods could aid with improving patient safety as well as reduce cost in emergency departments.
@drkohilathas - Dr. Eashwarran Kohilathas
The book was called Saving A&E The Toyota Way. I learnt a lot a about healthcare infrastructure, AI, and preventative medicine whilst researching for it. I knew what the national health situation was like, I knew we had to change as a species. https://amzn.eu/d/b5w6Upi
@drkohilathas - Dr. Eashwarran Kohilathas
I presented that book to my hospital, my consultants liked it, but as an acedemic piece. That was not my intention, but hey ho, life goes on. There were more pressing matters at hand. As the pandemic was progressing, I continued to research, write blogs and shared what I saw.
@drkohilathas - Dr. Eashwarran Kohilathas
And I saw a lot of unscientific rubbish, unethical practices and poor care. The reaearch papers said one thing, and yet we were doing something completely different. I knew from very early on that not everyone needed to be jabbed, something seemed fishy.
@drkohilathas - Dr. Eashwarran Kohilathas
I worked in the emergency department, and then paediatrics during the second peak. There was one child admitted due to C19 and later discharged. The ward was largerly empty. And yet many doctors online were saying that C19 was extremely dangerous to children. Nonsense.
@drkohilathas - Dr. Eashwarran Kohilathas
Something was off, doctors weren't being doctors, autopsies weren't being done, the medical field were ignoring anyone who didn't have C19, and yet staff were doing tiktok dances. They asked me to join. I refused.
@drkohilathas - Dr. Eashwarran Kohilathas
Whilst all this was happening, I lost my grandma. The docs didnt want to see her in her home, her infection got bad, she didn't want to go to hospital, she became septic, she had to go in. I visited her after my shifts and fed her during my breaks.
@drkohilathas - Dr. Eashwarran Kohilathas
On the night she died, I got a call from a doc with the bad news. I asked the doc if we could see her as a family, they approved. We saw her one after the other, in tears, trying to be quiet as to not wake the other patients up.
@drkohilathas - Dr. Eashwarran Kohilathas
Midway through, a matron I used to work with told us we couldnt see her due to hospital policy and warned us that if we carried on that she would call security on us. I told her we had approval already. She didn't care. I saw evil in her eyes.
@drkohilathas - Dr. Eashwarran Kohilathas
I asked her why she became a nurse. It was surely to treat and help people with compassion. She didn't budge. I said "go ahead and call security then". Thank God, we had enough time for our family to all say our goodbyes. I made sure I was the last one.
@drkohilathas - Dr. Eashwarran Kohilathas
I knew and saw that many others weren't as lucky as I was. Many had to facetime their dying family members. We were treated so badly. And healthcare professional encouraged it. I also knew the evils that lurked inside mankind that day.
@drkohilathas - Dr. Eashwarran Kohilathas
During paediatrics I asked my colleagues about masks and jabs. Why did we only allow one parent to see their newly born child whilst wearing a mask, but we could all snuggle up together in the staff room maskless, for example? I would get back parroted like responses.
@drkohilathas - Dr. Eashwarran Kohilathas
"It's the rules" "Policy" "To stop infection" "We just have to do it" No science. No debate. No convo. No brain.
@drkohilathas - Dr. Eashwarran Kohilathas
I later worked in a childrens psychiatric ward, and what I witnessed was truly backward. Many children, many who wanted to commit suicide, were placed in solitary confinement, so useless PCR swabs could be taken.
@drkohilathas - Dr. Eashwarran Kohilathas
Two would be need to be done and the nurses would sometimes forget to do these. I actually had to make them a table, so they would remember. Children had to be swabbed but staff members who'd go God knows where during the weekend didnt.
@drkohilathas - Dr. Eashwarran Kohilathas
I told my seniors that none of this made sense and children did not suffer with C19, but they just told me it was policy. The hospital trust actually recruited people to make sure staff were changing into scrubs before work too.
@drkohilathas - Dr. Eashwarran Kohilathas
The worst of it was when we had a wardround one time. In psychiatry the patient would sit in the room with the rest of the staff. This particular time, my consultant found out that the young person that was in the room with us wasn't swabbed.
@drkohilathas - Dr. Eashwarran Kohilathas
After the patient had left, she made us all stay in the room and asked us to lock the door and find ways to disinfect the room. She was seriously considering bleaching all surfaces. In disbelief, I asked her if we had to all strip down naked and shower together too.
@drkohilathas - Dr. Eashwarran Kohilathas
I had work to do, so I left. The mental health of children and adults during lockdown was the lowest I've ever seen it in my career. Children were arriving with life disruption related issues, trauma, abuse etc. All related to lockdowns.
@drkohilathas - Dr. Eashwarran Kohilathas
My next job was in general practice. I was working towards becoming a GP. I enjoyed understaning and looking after all sorts of patients. I'm a generalist at heart. However this transition marked another difficult time for me.
@drkohilathas - Dr. Eashwarran Kohilathas
On the last day of hospital medicine and just before the first day of GP, a close work colleague of mine went to play football, collapsed and never work up. Deep down I knew what had caused this. I knew the link between mRNA tech and myocarditis early on.
@drkohilathas - Dr. Eashwarran Kohilathas
I cried finding this information out. I cried in front of my mother for the first time in my adult life. I'm in fact tearing up typing this. My friend was killed.
@drkohilathas - Dr. Eashwarran Kohilathas
I went to his parents house to give my condolences. His parents were there, broken. He recently proposed to his fiancé. She was there too, broken. We viewed his funeral via Zoom.
@drkohilathas - Dr. Eashwarran Kohilathas
There's a spot in the park I dip in regularly whilst looking up at the leaves. I am reminded of him when I do this. I am reminded of how lucky I am to be alive. Deep down, I was terrified about what this meant for people around the world.
@drkohilathas - Dr. Eashwarran Kohilathas
Time went on, and I worked in general practice. There were murmurs of bringing in mandatory jabs to all healthcare staff. I knew this was not only unscientific and unethical, but murderous. Yet my colleagues didn't seem to care. They were safe I guess.
@drkohilathas - Dr. Eashwarran Kohilathas
Regardless I could not do anything about it, so I plodded along. I never stopped reading papers, writing, tweeting and sharing info. I saw patients, I saw jab related side effects, missed periods, new onset whole body inflammation, hair loss etc. I saw cognitive dissonance too
@drkohilathas - Dr. Eashwarran Kohilathas
All of a sudden, one day, my practice asks me my full jab status. I find this odd because they knew I had to be jabbed with everything else to have worked in all the other specialties. I knew they wanted to know only one result. Whether or not I had taken the C19.
@drkohilathas - Dr. Eashwarran Kohilathas
I didn't lie. Told them the truth. The next day, in a panic, they asked me to stop seeing patients face to face. They had made a decision as a team, without me, that I was no longer able to see patients. They felt that I wa a threat to them and I would scare them away.
@drkohilathas - Dr. Eashwarran Kohilathas
I have never had C19, I worked on my health and immunity every day and I purposely breathed in the virus in ED to stimulate T cells. I knew jabs increased ones risk of infection and showed them evidence. I was the least risky person in the practice and I knew it.
@drkohilathas - Dr. Eashwarran Kohilathas
They didn't care. They didn't care about evidence. They didn't care about ethics. About immunity. About anything. I shrugged this off and called patients instead. I was ostracized at work and many colleagues acted cold towards me. I was alone, but not lonely, I had science.
@drkohilathas - Dr. Eashwarran Kohilathas
Many doctors had to take sick leave off work due to C19 multiple times. I had meetings discussing my jab status. A doc with myocarditis on long term meds lost jab urged me to get the shot. One said I was "too principled" It was surreal.
@drkohilathas - Dr. Eashwarran Kohilathas
They admitted it was all politics. I asked them why they didn't read papers? I asked them about T cells? Silence.
@drkohilathas - Dr. Eashwarran Kohilathas
I wanted to become a doctor since the age of 6. I love biology and enjoy helping people using my knowledge. But I understood that I was getting stupider and working in an environment that was harming people. I had many sleepless nights thinking about leaving.
@drkohilathas - Dr. Eashwarran Kohilathas
One morning, after parking my car at work, I felt a warmth around my head. It had no words, but if it did it told me that everything will be okay. As soon as I had that experience, my decision was made and I felt light, a colossal weight had been lifted.
@drkohilathas - Dr. Eashwarran Kohilathas
I asked to quit, and a few meetings later (carried out to make sure I wasn't crazy), I left healthcare and then deregistered myself off the medical register. I wanted to be totally free. I needed to be.
@drkohilathas - Dr. Eashwarran Kohilathas
The flat my girlfriend and I were planning to buy fell through. I was in financial turmoil. My mother cried for weeks. I was lost, but I was free. I wasn't part of the killing system.
@drkohilathas - Dr. Eashwarran Kohilathas
I did what I only knew, I began writing. I started a Patreon and am grateful for those who did and continue to contribute to that. But it wasn't enough. I ended up being on the dole for just less than a year. The guy I had to call every 2 weeks was surprised I was once a doc.
@drkohilathas - Dr. Eashwarran Kohilathas
I began learning and researching everything I could to help people who had been jabbed I knew what was going on and I didn't want another pandemic to happen. I wanted to save as many lives as possible.
@drkohilathas - Dr. Eashwarran Kohilathas
I would take my bike, cycle across the park to my local library and work feverishly every day till close. Around this time I was permanently suspended on Twitter for stating facts.
@drkohilathas - Dr. Eashwarran Kohilathas
I see this as a blessing now, as it made me work even harder to produce something that could never be banned. A book. I worked and researched to make sure I got this book out before 2023.
@drkohilathas - Dr. Eashwarran Kohilathas
I was blessed around this time to come in contact with @ake2306 , he introduced me to other people injured by the shots. I was determined to make sure their voices got heard. I included their stories in the book.
@drkohilathas - Dr. Eashwarran Kohilathas
During this time on my walks, I experienced many insights and extraordinary experiences that many may not believe or call me crazy. I saw light, and I ended my fears.
@drkohilathas - Dr. Eashwarran Kohilathas
Before the new year, I released my book, "Calling Out The Shots" It goes through what genetic agents are, what they do to our bodies, how we can improve our immunity, ways we may mitigate jab damage and what we need to do as a society to heal. http://www.callingouttheshots.xyz
@drkohilathas - Dr. Eashwarran Kohilathas
My only aim now is to help heal and free mankind. To me, it is the most important book ever written. Even if I am killed, the book will live.
@drkohilathas - Dr. Eashwarran Kohilathas
The book marks my first gift to the world. I am working on many more, and other projects. I will fight for humanity until my final breath.
@drkohilathas - Dr. Eashwarran Kohilathas
Through my toils I have come to know some extraordinary people. Though I have seen and experienced evil. I have also seen God and light in mankind as well. I know we will be alright.
@drkohilathas - Dr. Eashwarran Kohilathas
They've banned me multiple times. What's stopping them from banning me again? To always stay in the loop. Please subscribe 🙏🏾 https://www.drkohilathas.co.uk/subscribe

@drkohilathas - Dr. Eashwarran Kohilathas
Just woke up, my mind is racing, it makes sense having to reflect on everything that has happened over the last few years. I obviously haven't mentioned everything I witnessed. Maybe I'll use this thread jot down events that happened as I remember them again.
@drkohilathas - Dr. Eashwarran Kohilathas
One thing I failed to mention was the day I lost complete trust in the GMC, the UK medical regulatory body, supposedly in charge of protecting patients from doctors. I remember when plans on introducing the jabs to children nationally was considered. I was mortified.
@drkohilathas - Dr. Eashwarran Kohilathas
I knew through real life and via scientific evidence that children did not need these jabs whatsoever. So in desperation I wrote an open letter to the GMC, highlighting all the evidence, basically pleading with them to reconsider the roll out.
@drkohilathas - Dr. Eashwarran Kohilathas
I was putting my career at risk by doing this. I knew I would become a target. But I didn't care. We were talking about childrens lives.

@karthik2k2 - Karthik Endocrinologist
While joining MBBS in 2023 is a bad idea for anyone , it’s particularly stupid for a Tamilnadu student. Why ? A 🧵
@karthik2k2 - Karthik Endocrinologist
In PG there’s a service quota occupies a big place in a complex matrix of reservation. If you don’t have rich parents, you may need to join some PHC job to improve your chances of PG - thereby wasting time
@karthik2k2 - Karthik Endocrinologist
Tamilnadu is quite possibly the worst place for a doctor in India - since it’s hyper saturated with doctors. Given that incubation period of a super specialist is 12 to 15 years, that many more would have joined the workforce when you complete.
@karthik2k2 - Karthik Endocrinologist
The direct consequence of excess supply without proportionate demand is low pay. Even if you do MD and DM from the finest institutes, you will still be paid peanuts compared to your peers in other states.
@karthik2k2 - Karthik Endocrinologist
Perhaps you think you can go to some other state? Good - but due to decades of language politics, most Tamils don’t speak Hindi- this includes doctors too. For a dr from Jaipur going to Lucknow is easier - like it’s easier for a Tamil to go from Madurai to Trichy
@karthik2k2 - Karthik Endocrinologist
Sure you can learn the language - but someone who already knows it is more attractive to an employer and you/ your family s comfort level is low in another state. Between a small town in TN or a corporate hospital in another state, you may end up choosing the former
@karthik2k2 - Karthik Endocrinologist
There are other exit routes - like USMLE or PLAB. USMLE needs financial backup. If you don’t have a solid back up, it may not be an option unless you are willing to ask your parent to take debt on your behalf
@karthik2k2 - Karthik Endocrinologist
At this point you may be tempted to ask- doesn’t engineering suffer from the same problem? The average engineer also earns less? Yes - but you are comparing apples to oranges. The avg govt college medico is the creme de la Creme, the best in his school/ class.
@karthik2k2 - Karthik Endocrinologist
So it only makes sense to compare avg medico to engineers from the top colleges. The engineers have better exit routes without having to slog for a decade. You can check out apps like Glassdoor or Fishbowl for better idea
@karthik2k2 - Karthik Endocrinologist
A simple comparison of salary is not enough. Compare the social milestones too - the age at marriage, first child, getting a home, car or first vacation abroad. Doctors lag behind in every one of these. Of course this is not limited to TN- then why is it relevant?
@karthik2k2 - Karthik Endocrinologist
Doctors elsewhere can make up for the lost ears by earning more. In TN that’s unlikely, unless you have an entrepreneurial bent of mind along with capital and connections. If not you don’t have a catch up phase to bank on.
@karthik2k2 - Karthik Endocrinologist
Finally , if you are in to politicking govt jobs are a good option - if not they are not. In any case, govt jobs aren’t easy to come by.
@karthik2k2 - Karthik Endocrinologist
Getting a seat in an institute of national importance ( AIIMS, PGI, JIPMER etc) may at least make you feel better - since fees is low. But that’s like coming to Chennai with the idea of becoming an actor - too much uncertainty
@karthik2k2 - Karthik Endocrinologist
In short there is hardly any upside to doing medicine if you are in TN. Unless you are extremely passionate it’s foolhardy to take medicine if you are from TN. You will be better off doing anything else - since you are a top class student anyway.

@houmanhemmati - Houman David Hemmati, MD, PhD
There's been a lot of recent attention on #DEI in college admissions thanks to @GovRonDeSantis @RonDeSantisFL pushing to ban DEI-based admissions in Florida & to DEI in medicine w/@IngrahamAngle @wsj @nypost reporting on @AAMCtoday adding DEI to medical schools. But the scope of DEI in medical school admissions hasn't been known by the general public. As a former admissions committee member of a top-20 med school, I was shocked to learn how much med schools have recently shifted away from merit & questions about "why medicine" goals as a physician to overtly DEI-based admissions questions. Here's what I have found:
@houmanhemmati - Houman David Hemmati, MD, PhD
Of all the allopathic (MD) and osteopathic (DO) medical schools in the United States, the majority have questions on their 2022-2023 application cycle applications that relate to “DEI” issues. Typically, the question is: “How would you contribute to the diversity of our medical school.” For someone who doesn’t meet the currently-accepted definition of “diversity”, that’s already a hard enough question to answer. Yet many med schools go (far) beyond basic DEI to ask about identity, sexual orientation, anti-racism and proof that the applicant is committed to social justice issues. These questions are used to screen and weed out applicants. If you don’t pass, you won’t get an interview and your application is dead.
@houmanhemmati - Houman David Hemmati, MD, PhD
A for-profit admissions advising site has done a great job of publishing every medical school’s 2022-2023 secondary (school specific) application questions. They’re located here (I have no affiliation with the site/company): https://www.shemmassianconsulting.com/blog/medical-school-secondary-essay-prompts

@houmanhemmati - Houman David Hemmati, MD, PhD
Here’s a list of US med schools that I found to contain at least one DEI question on their application. Note that many are surprisingly in “red” states like FL and TX where you’d least expect it: Alabama College of Osteopathic Medicine University of Alabama School of Medicine University of South Alabama College of Medicine University of Arizona College of Medicine – Phoenix University of Arizona College of Medicine – Tucson Arkansas College of Osteopathic Medicine California Health Sciences University College of Osteopathic Medicine California Northstate University College of Medicine California University of Science and Medicine School of Medicine Kaiser Permanente School of Medicine Stanford University School of Medicine University of California – Irvine School of Medicine University of California – Riverside School of Medicine University of California – San Francisco School of Medicine University of Southern California Keck School of Medicine Western University of Health Sciences College of Osteopathic Medicine Yale School of Medicine George Washington University School of Medicine and Health Sciences Georgetown University School of Medicine Florida Atlantic University Charles E. Schmidt College of Medicine Florida International University Herbert Wertheim College of Medicine Florida State University College of Medicine University of Central Florida College of Medicine University of South Florida Health Morsani College of Medicine Medical College of Georgia at Augusta University Mercer University School of Medicine Chicago Medical School at Rosalind Franklin University of Medicine and Science Loyola University Chicago Stritch School of Medicine Northwestern University The Feinberg School of Medicine Rush Medical College of Rush University University of Iowa Carver College of Medicine* University of Kansas School of Medicine University of Kentucky College of Medicine University of Louisville School of Medicine Tulane University School of Medicine Johns Hopkins University School of Medicine Uniformed Services University of the Health Sciences F. Edward Hebert School of Medicine University of Maryland School of Medicine Harvard Medical School Tufts University School of Medicine University of Massachusetts Medical School Michigan State University College of Human Medicine Oakland University William Beaumont School of Medicine University of Michigan Medical School Western Michigan University School of Medicine Mayo Clinic Alix School of Medicine University of Minnesota Medical School William Carey University College of Osteopathic Medicine Saint Louis University School of Medicine University of Missouri – Columbia School of Medicine University of Missouri – Kansas City School of Medicine Washington University School of Medicine Geisel School of Medicine at Dartmouth Hackensack Meridian School of Medicine Rutgers New Jersey Medical School Columbia University College of Physicians and Surgeons Icahn School of Medicine at Mount Sinai New York Institute of Technology College of Osteopathic Medicine New York Medical College SUNY Downstate Health Sciences University College of Medicine Stony Brook University Renaissance School of Medicine University at Buffalo Jacobs School of Medicine Duke University School of Medicine University of North Carolina at Chapel Hill School of Medicine Cleveland Clinic Lerner College of Medicine The Ohio State University College of Medicine Oregon Health & Science University School of Medicine Geisinger Commonwealth School of Medicine Philadelphia College of Osteopathic Medicine Sidney Kimmel Medical College at Thomas Jefferson University University of Pennsylvania Perelman School of Medicine University of Pittsburgh School of Medicine Brown University The Warren Alpert Medical School University of South Carolina School of Medicine – Columbia University of South Dakota Sanford School of Medicine East Tennessee State University Quillen College of Medicine (Continued)…
@houmanhemmati - Houman David Hemmati, MD, PhD
University of Texas Medical Branch School of Medicine University of Texas Rio Grande Valley School of Medicine University of Texas Southwestern Medical School University of Utah School of Medicine University of Vermont Larner College of Medicine Eastern Virginia Medical School University of Virginia School of Medicine Washington State University Elson S. Floyd College of Medicine University of Washington School of Medicine Medical College of Wisconsin University of Wisconsin School of Medicine and Public Health
@houmanhemmati - Houman David Hemmati, MD, PhD
Among these DEI-focused med schools, there are some that take DEI to an entirely new level, making you wonder whether they’re recruiting future doctors or future social justice warriors like the PhD social justice “doctor” Barbara Ferrer who leads @lapublichealth Take @StanfordMed which asks: “The Committee on Admissions regards the diversity (broadly defined) of an entering class as an important factor in serving the educational mission of the school. You are strongly encouraged to share unique attributes of your personal identity, and/ or personally important or challenging factors in your background. Such discussions may include the quality of your early education, gender identity, sexual orientation, any physical challenges, or any other life or work experiences.”
@houmanhemmati - Houman David Hemmati, MD, PhD
Or @UCIMedSchool which asks “Do you identify as being part of a marginalized group socioeconomically or in terms of access to quality education or healthcare? If so, please describe how this inequity has impacted you and your community.” @dgsomucla echoes those themes by asking “Do you identify as being part of a group that has been marginalized (examples include, but are not limited to, LGBTQIA, disabilities, federally recognized tribe) in terms of access to education or healthcare? (Yes/No) •If you answered “Yes” to the above, answer the following prompt: Describe how this inequity has impacted you or your community and how educational disparity, health disparity and/or marginalization has impacted you and your community.” Not wanting to be left out, @UCSFMedicine asks “Do you identify as being part of a marginalized group socioeconomically or in terms of access to quality education or healthcare? Please describe how this inequity has impacted you and your community.” And @KeckMedUSC simply asks “Are you a member of a group that is under-represented in medicine? (Yes/No) •If yes: Which Group? How does under-representation affect your community? “ Notice a pattern? If you’re not oppressed or marginalized in their particular way, you’re not as worthy.
@houmanhemmati - Houman David Hemmati, MD, PhD
It gets interesting from here. @WesternU won’t let you apply unless you think DEI is “important” by asking “What does diversity, equity, and inclusion mean to you and why are they important? “ Not to be undone, GWU in DC asks “Describe how current issues regarding advocacy and social justice have impacted your motivation for medical school?” Too bad if you want to be a doctor to just help sick people or keep people healthy. While other med schools like @FSUCoM in Florida care a lot about identity by asking “If there is an important aspect of your personal background or identity, not addressed elsewhere in the application, that you are comfortable voluntarily sharing with the Committee, we invite you to do so here. Many applicants will not need to answer this question. Examples might include significant challenges in access to education, unusual socioeconomic factors, identification with a minority culture, religion, race, ethnicity, sexual orientation or gender identity. Briefly explain how such factors have influenced your motivation for a career in medicine.”
@houmanhemmati - Houman David Hemmati, MD, PhD
U Kansas continues the identity theme by asking applicants “Please tell us about your identity. How has your identity impacted the development of your values and attitudes toward others, particularly those with values different from your own? Please include how your values and attitudes will foster a positive learning environment during your training, and benefit your future patients through the practice of medicine.” Can you apply if you identify as a human? Such factors also matter to U Kentucky which asks “Please share unique, personally important, and/or challenging facts in your background, such as the quality of your early educational environment, socioeconomic status, culture, sexual orientation, race, ethnicity, or life/work experiences. Please discuss how such factors have influenced your goals and preparation for a career in medicine.”
@houmanhemmati - Houman David Hemmati, MD, PhD
Interestingly, U Louisville makes it clear that certain non-diverse cultures are less capable of delivering “equitable care” when they ask “How have your cultural experiences shaped the way you see yourself contributing to the medical field and strengthened your ability to provide equitable care for a diverse patient population?” @TulaneMedicine asks the seemingly bread and butter DEI question “Tulane University School of Medicine values the diversity of its patients, faculty, staff, and students. Do you identify with a particular group that you believe is underrepresented among medical professionals? These include groups oriented around, but nt limited to: ethnicity, race, sexuality, religion, disability, and economic background.” The military medical school even gets in on it when @USUhealthsci overtly invokes DEI in their application by asking “Our Admissions Committee assembles classes of students with a wide range of backgrounds, skills, experiences, and talents. Please describe how a special quality or experience of yours has informed your ability to participate well in a diverse, equitable, and inclusive environment.”
@houmanhemmati - Houman David Hemmati, MD, PhD
@harvardmed at least acknowledges that not every applicant will meet the DEI litmus test by saying “If there is an important aspect of your personal background or identity, not addressed elsewhere in the application, that you would like to share with the Committee, we invite you to do so here. Many applicants will not need to answer this question. Examples might include significant challenges in access to education, unusual socioeconomic factors, identification with a minority culture, religion, race, ethnicity, sexual orientation or gender identity. Briefly explain how such factors have influenced your motivation for a career in medicine.”
@houmanhemmati - Houman David Hemmati, MD, PhD
Med schools in Michigan are aboard the DEI and systemic injustice train as well! @michiganstateu asks “American society may be experiencing a watershed moment as it reckons with various systemic injustices. Use the space below to share your thoughts about this statement.” And @UMichMedSchool has a two-parter with “•Describe your identity and how it has impacted the development of your values and attitudes toward individuals different from yourself and how this will impact your interactions with future colleagues and patients. •If you recognize and/or represent a voice that is missing, underrepresented, or undervalued in medicine, please describe the missing voice(s) and how increased representation in medicine could impact the medical community.”
@houmanhemmati - Houman David Hemmati, MD, PhD
The hands-down winner of the med school admissions DEI contest is @umnmedschool in Minnesota with its EPIC DEI application and DEI-driven “pathways” that segregate students based on identity: “Describe a time when you personally experienced, observed, or acted with explicit bias. What did you learn about yourself and the experience? The University of Minnesota Medical School is committed to building an anti-racist community. Please share your reflections on, experiences with, and greatest lessons learned about systemic racism. (Consider this country's history, racism, racial injustice, anti-black racism, and the impact of the murder of Mr. George Floyd on the Minnesota/Twin Cities community). How will your unique attributes (religion, race, ethnicity, socioeconomic status, ideology, intellectual heritage, and/or experiences) add to the overall diversity of the University of Minnesota Medical School community? Select your pathway interest(s) below (you may select more than one). Once you make your selection there will be additional questions that you will be required to answer •Indigenous Health Pathway •Rural Health Pathway •Urban Communities Pathway •2SLGBTQIA+ Pathway: The University of Minnesota Medical School is committed to dismantling the health disparities affecting Minnesota’s 2SLGBTQIA+ communities. Describe your experiences engaging and/or working with 2SLGBTQIA+ communities and explain why 2SLGBTQIA+ inclusive health care is important •Immigrant | Refugee | Global Health Pathway”
@houmanhemmati - Houman David Hemmati, MD, PhD
And this continues with @MOmedicine asking “"How will your diversity/diverse experiences (e.g., gender, gender identity, race, ethnicity, sexual orientation, veteran status, from rural or underserved community, first generation student status) add to your career in medicine?" And @WUSTL similarly asks “Is there anything else you would like to share with the Committee on Admissions? Some applicants use this space to describe unique experiences and obstacles such as significant challenges in access to education, unusual socioeconomic factors, and/or identification with a particular culture, religion, race, ethnicity, sexual orientation, or gender identity and/or possibly challenges related to COVID or other issues in preparation for medical school.”
@houmanhemmati - Houman David Hemmati, MD, PhD
@GeiselMed at @dartmouth has an interesting DEI question: “Geisel School of Medicine values social justice and diversity in all its forms. Reflect on a situation where you were the “other.”” Are you allowed to answer with “When I applied to med school as a non-diverse applicant”?
@houmanhemmati - Houman David Hemmati, MD, PhD
The most shocking example of a med school overtly threatening to CANCEL you and rescind admission or kick you out if your PAST OR PRESENT social media presence has ever said anything offensive is New York Medical College (which even has a @Diverse_NYMC Twitter account) that actually says (not a joke!): “Please review the NYMC Social Media Policy. If you select YES, we ask that you please briefly explain what has been posted. In keeping with New York Medical College’s (NYMC) and Touro College and University System’s policies on prospective student online conduct, College staff members do not “police” online social networks and the College is firmly committed to the principle of free speech. However, when the College receives a report of inappropriate online conduct, we are obligated to investigate; New York Medical College reserves the right to rescind admissions for misconduct or lack of professionalism wherever it occurs, including online. Is there anything in your social media presence (past, or present) that would bring discredit or dishonor on you, the institution, the program or profession (if applicable) or that could be considered derogatory, hateful, or threatening? (Yes/ No)” WHAT?!? I think they made this for @kevinnbass 😂🤣
@houmanhemmati - Houman David Hemmati, MD, PhD
@StonyBrookMed doesn’t give you the option to say “none” when they ask “What, in your opinion, is the role of a physician in addressing systemic racism and societal injustices?” And @OHSUSOM REALLY wants to make sure you understand and adhere to their definition of diversity: “Please discuss how your personal experience demonstrates the ability to overcome adversity and contributes to diversity in the provision of healthcare. Please include any insight into the diversity that you would bring to OHSU School of Medicine and the profession of medicine in the context of OHSU's definition of diversity: Diversity at OHSU requires creating and sustaining a community of inclusion. We honor, respect, embrace and value the unique contributions and perspectives of all employees, patients, students, volunteers and our local and global communities. Diversity may include age, color, culture, disability, ethnicity, gender identity or expression, marital status, national origin, race, religion, sex, sexual orientation, and socioeconomic status. We respect diversity of thought, ideas and more. Diversity maximizes our true potential for creativity, innovation, quality patient care, educational excellence and outstanding service.”
@houmanhemmati - Houman David Hemmati, MD, PhD
In comparison to other DEI med schools, @GeisingerCwlth seems boring when they only ask “Geisinger Commonwealth values diversity and is committed to maintaining an inclusive environment. How will you contribute to our commitment to diversity, social justice, equity, and inclusion?”
@houmanhemmati - Houman David Hemmati, MD, PhD
In another example of “Did they really say that?!” Philadelphia College of Osteopathic Medicine actually comes out and asks “PCOM recognizes and affirms the dignity of all members of the PCOM community. Do you self-identify as part of the LGBTQIA community? (Yes/No) •If yes, please use this space to specify your identity within the LGBTQIA community, if you wish.” Wow. Just wow.
@houmanhemmati - Houman David Hemmati, MD, PhD
Finally, in Texas, @utmbhealth asks “John Sealy School of Medicine values inclusion and advocacy. Describe a time when you advocated for someone whose social identity (e.g., race, gender, sex, sexual orientation, religion, socioeconomic status, ability status, etc.) differed from yours. Explain the situation and why advocacy was necessary” & @UTHealthRGV (@BillFOXLA stomping grounds) asks “The University of Texas Rio Grande Valley School of Medicine has commitments to diversity, inclusion, and health equity. What do these terms mean to you? What is their importance to medical education and practice, as well as to the health of our society in general?” Finally, @UofUHealth asks “ The School of Medicine aims to create a culture of inclusion and anti-racism in health education and healthcare delivery. How have you promoted or advocated for health equity in your experiences? How do you envision contributing to the UUSOM and the communities we serve?”
@houmanhemmati - Houman David Hemmati, MD, PhD
We need to ask whether these DEI admissions questions/policies, which are so obsessively focused on sexual orientation, gender identity, skin color and other factors, do anything to create doctors who deliver better care. Back in my day, med schools believed that any good person could be trained to take care of any patient, regardless of who they are, by treating every human with equal value, equal compassion, and an equal commitment to better health. Do doctors now really need to look and/or act like their patients to deliver them quality care? Sure, there can certainly be cultural and language benefits in many cases, but med schools are clearly going beyond that by selecting for progressive social justice activists and people with “diverse” identities rather than focusing on who is going into medicine for the right reasons and who is most likely to perform well in the future. It’s time for a serious discussion about this.
@houmanhemmati - Houman David Hemmati, MD, PhD
@foxnewsnight @tracegallagher @BrigidMaryMcD @TuckerCarlson @DrJBhattacharya @RupaliChadhaMD @afshineemrani @drlitvack @cabot_phillips @benshapiro @ToddPiro @SteveHiltonx @megbasham @MorningInUSA123 @mattbilinsky @hamill_law @AppletoZucchini @akheriaty @PeterDiamandis @elonmusk @StellaEscoTV @AzadehKhatibi @SabinehazanMD
@houmanhemmati - Houman David Hemmati, MD, PhD
@ShellenbergerMD @mtaibbi @bariweiss

@kacdnp91 - Kelly DNP🩺 Functional Med
The critical thinkers will be nonexistent in healthcare. All by design. https://t.co/gVLmCbMW98


@goddeketal - Dr. Simon Goddek
🎓 THE COLOSSAL DOWNFALL OF ACADEMIA I obtained my PhD from one of the best universities in the world, but eventually lost my position there for questioning how the Covid PCR protocol publication managed to pass the peer-review process in less than one day. To phrase it differently, this scenario is like your 90 years old grandmother challenging Usain Bolt to a 100m race and beating him by several seconds. The likelihood of this occurring is zero. Imagine that all sports experts would mock you if you contested the result, even though the facts are clear. The same scenario played out across all global 'elite universities.' Despite the availability of facts and data, no institution dared to analyze them and draw conclusions that diverged from the political mainstream. The paramount question is why did not a single 'elite university' dare to remark that: ▪️These Covid vaccines are 'gene therapies.' ▪️These gene therapy vaccines contain bacterial DNA contamination, which has led to cancer in other gene therapy trials. ▪️These gene therapies do not prevent infection. ▪️These gene therapies do not halt the 'spread.' ▪️These gene therapies have not been shown to have any clinical benefit. ▪️These gene therapies have caused the most confirmed direct deaths in the history of any medical product. ▪️These gene therapies do cause serious adverse events (SAEs) at a rate of at least 1 in 800, and are based on a sequence that has never been validated. ▪️These gene therapies are solely a reaction to the PCR test pandemic fraud of 2020. ▪️These gene therapies contain highly inflammatory liposomal nanoparticles (LNPs). ▪️These gene therapies did not stop excess mortality. So what are these 'elite universities' actually good for? Indoctrination? Creating modern slaves burdened with tens or hundreds of thousands in tuition fees? One thing is for sure - schools and universities are no longer bastions of critical thinking, but rather tools of the elite to avoid critical thinkers. Those who think critically are weeded out, like me, while those who constantly support the current narrative are promoted to professorships. Brave new world!

@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Hearings for BC Nurse Amy Hamm @preta_6 begin again at 1pm est/10am pacific today. #FreeSpeech Will @JamesCantorPhD (one of Canada's top researchers in atypical sexuality & paraphilias) be accepted as an expert witness for Hamm? find out w/ me. I'll be🧵ing
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
and we're back on the record... @bastow_karen opens. It seems that Cantor has been accepted as an expert witness & will be examined by Bastow then subject to cross examination. Next Witness will be Amy Hamm, and @LDBildy will be calling witnesses for Hamm next week.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Dr James Cantor is taking the virtual stand, swearing in. Bastow taking Cantor through his report prepared for the Amy Hamm hearings: Some repetition of the qualification process as Cantor testifies now to his qualifications. BARBARA FINDLAY objects to Cantor's statement of qualifications... Panel ruling was to limit testimony to gender dysphoria and gender identity Bastow qualifies her opening question: Cantor is entitled to testify to his overall experience but Bastow will limit to GD and Gender Identity expertise
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor: Diagnostic criteria for intervention for GD has changed in the last twenty years. Quote: "Standards are not standards if they are open to interpretation" We moved away from gatekeeping model (attempts to mitigate harm was a long process of months or years living as desired self) to an informed consent model. There is no strong evidence for benefits for intervention in transition. This must be Informed consent model is a general model for physically evidenced disease. Is the person cognitively capable of making decisions?
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Bastow: does the informed consent model apply kids under 16 in Canada? Cantor: it's complicated. Generally requires the involvement of parents unless parents do not consent... Bastow: asking about US gatekeeping... moves on to Europe... FINDLAY (objection): asks that Dr. Cantor/panel to restrict testimony to Canada and the US models Bastow responds: Science is not limited by geography. Science is not confined by the legal jurisdictions. Decisions of other countries are relevant to the testimony. Panel stands down for five minutes.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Panel agrees that Bastow can pursue the question: "can you advise us on the position of various European countries over 16 and under 16 - and whether models have changed in this are since 1998." Europe has gone in opposite direction of Canada and US. Originally went in the same direction but quickly realized treatments were not having the desired organizations. Europe rejectected WPATH and activist positions and now explicitly reject treatments under informed consent. Is exact opposite direction of Canada and US. Europe has controlled for and removed people with conflict of interest... Cantor points out well-known conflict of interest are both financial and biased towards benefiting certain specialties
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor elucidating on conflict of interests - if practitioners and clinics are positioned to benefit from the medical interventions and they are the only ones creating the guidelines. Europe has figured this out and is having reviews independent of the specialties that benefit from financial and intellectual conflict of interest. Conflicted groups in the US are coming up with policies that benefit them. These specialties should not be in charge of developing guidelines. My words: this is like putting the fox in charge of the henhouse.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
WPATH uses sketchy language to describe development of policies and conflict of interest. Claims no-one is in a conflict of interest at WPATH. Bastow: Q re: conflict of interest Cantor: WHO and National Academy counts that being the recipient of a grant in a specialty, or providing services in this speciality puts the recipient in a conflict of interest for policy development. This means that WPATH development of guidelines is outside of internationally recognized rules of conflict of interest.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Bastow: Can you elaborate on change of demographic. Cantor: occurred in every country. the change exploded in 2012 (coincidentally?) was same year WPATH changed guidelines. Demographic changes Europe, US and Canada, explosive change was primarily in youth, was mostly male who would grow to young gay men. the change was mostly male for several decades, after social media it became a different cohort, biologically female, early adolescent and onset of puberty Different mental health profile. Can't assume the same protocols used for previous cohort should apply Also the male presenting adults, AGPs after 2012, no longer subject to gatekeeping either.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Bastow: why is gatekeeping important with AGP? Cantor: it is well established that biological men, adult onset GD have a sexual interest pattern that is more unusual than being gay or lesbian, men attracted to self as female. unlike gay kids effeminate, these are often married straight. AGP occurs with other sexual interests, clinical question: are men taking advantage of transgender identities in order to act out their other interests like exibitionism or sadist taking advantage of the situation in order to enact the other What are the motivations of of the client? When self-identification is the only criteria and there is no objective evaluation then people can take advantage of society's willingness to embrace sexual diversity
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Bastow: have service levels increased or decreased Cantor: amount of energy has not gone down but there is a question of this is sapping away from resources for general mental health for, let's say, teenagers.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Bastow: Drugs, can you speak to the types of drugs and use of drugs in the treatment of gender dysphoria. Cantor: Lupron is same drug as the drugs used euphemistically as chemical castration drugs Primary long-term side-effects are bone density loss and osteoporosis.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Bastow: you've had experience in research design, also as senior scientist at CAMH - can you expand on designing research into sexual behaviour. Cantor, you've just described a course I might teach. From full range of scientific methods, from hardcore math and physics and design of questionnaires... Can tell you strengths and weaknesses of research designs.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor confirms he has reviewed Hamm's comments as well as investigative reports of Hamm's comments. Bastow: moving into new area... taking a break: return at 11:30/2:30 est
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Back on the record. #iStandWithAmyHamm Fellow Xweeps: what is important to you about the outcome of these hearings? Do you think if Hamm is exonerated this will make a difference in Canada and alleviate some of the fear related to being witch-hunted?
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Bastow: can you state your summary of opinions excepting redactions from your report Cantor: Opinions are are unchanged & the facts available regarding the importance of speaking out against their own clinics. American Academy of Pediatrics is subject to a lawsuit, and is undertaking a systematic evidence review Hamm's comments include statements that people don't want to hear, science and society must contain examples of speaking out about the issue and about science itself. growing evidence and growing voices critical of the practices
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor: people are relying on perceptions and subjective feelings. People are preying on others based on emotions and claims of victimization. Bastow turning to: "No consensus among clinicians on best methods of treatment the primary theories of what's going on. Agreed Upon: enormous and increasing need for MH services, & many people presenting with GD People accept at face value vs people relying on objective evidence. So much emotion, so few experts, so much conflict of interest, & people are making decisions based on optics and political posturing. Public discussion consists of half truths, omissions of relevant information, Objectivity has come to opposite conclusion of what is popular. International orgs have come up with same conclusion, but US & Canada are opposite. Making decisions based on optics rather than verifiable truths.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Pyramid of Evidence Cantor: how to distinguish between good science and bad science one set of studies vs another set of studies for non-scientific boards of decision-makers. The purpose of the pyramid or levels of evidence is to rank quality of evidence. transition on demand relies on low-level studies. Ignore higher level studies that outrank the lower level studies. ie surveys correlation does not imply causation
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor compares magic ritual over crystals causing the a lucky day the next days to the quality of poor/low level studies. Correlation is not causation. Best evidence is from Randomized Controlled Trials (RCT) Next a cohort study is taking a group and track them over time. We're seeing the same people over time so we get to watch for differences.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor: No RCT studies have been conducted for treatment for GD. The best we have is the cohort study. The very highest level is the systematic reviews of evidence (meta study) Bastow: There is no evidence indicating any consensus. We can only tolerate strong risk when we have strong evidence. Bastow: could you comment on how gay men might be disadvantaged by current protocols. Cantor: unanimous studies show most effeminate boys grow out of dysphoria. Young gay men are put in danger by current policies. Bastow: how are women disempowered by current policies? Cantor: adult onset type (male attracted to women) are more ambiguous of what's motivating them interfering with women and their sense of safety. Bio males present more perceived risk. Locker rooms, adult males with atypical interest also exhibit more than one atypical sexual interterest. Impossible to know what the motivators are.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Bastow: how does ROGD relate to the disempowerment of women. Cantor: childhood onset strongly related to homosexuality; adult type strongly related to atypical sexualities. ROGD is a third group emerged with social media, at same time as spike in mental health issues in children in retrospect it seems obvious.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor: people are generalizing treatments from other groups (childhood onset & adult onset) to the mostly female cohort of adolescent onset there is nothing to say that the treatments for one or both (very rare) classical types would work for the new very common presentation of teenage girls. Current policies are preventing young women from developing healthy identities that would be normal for young women.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
today is a hearing day for @preta_6 Amy Hamm's hearing Dr James Cantor testifying. Points out the definition of Experimental prevents insurers from paying for intervention. So Orgs like WPATH make assertions / opinions that these protocols are NOT experimental. Bastow: can you go through the terms of art about sex vs gender? Cantor: largely on Social Media, use sex and gender in ways not related to science Once can determine one's sex with a reliability better than almost any other trait difference. The definition of sex has been, many writers take the list of objective verifiable characteristics simply ad gender identity to the list of descriptors related to sex. "gender" has a long history of being defined in amorphous terms.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor now going into DSDs disorders of sexual development. Cantor goes into various presentations of DSDs. DSDs are exceptionally rare, less than 1/10th of 1% of we exclude hypospadia (a birth defect in males where the urethra does not open at the head of the penis)
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
We are back again with the hearings for @preta_6 with the BC College of Nurses & Midwives. There have been many developments in the issue in the public domain. One of them is the obvious correlation between gender activism & open anti-semitism of the radical woke cancel-cult left; another is the Angus Reid polling on the culture wars showing how small a population the cancelt cult left is. Back on the record:
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor: Another correlation with the Adolescent Onset GD, they have other disorders, ASD, Personality Disorder and Histrionic Disorder. They have social functioning disorders developing healthy social functioning. not getting the same attention as the flashy, easy-to-retweet superficial interpretation of GD In science there is no such thing as inner sense. Science requires something be falsifiable. requires something basic to be scientifically verifiable. Even depression shows (vague) but verifiable patterns in brain scans, but self-reported gender identity cannot be verified. #IStandWithAmyHamm
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor: Science has verified evidence of gay and lesbian brains, when we take groups and compare them, there is evidence of being shifted towards the opposite brain. Several studies have made mistakes when trying to verify a trans brain. "Confounding" problem examined mutli-variant subjects (gay and also trans) and confounded the differences. the conclusions in the studies could not be stated clearly because we couldn't verify gender identity in the brain. (I've been reading & studying on this subject for years and this is just the clearest articulation of this claims and science I've ever heard - partly why I'm taking these notes in detail)
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor: integration of sexual orientation into society & integration gender identity into society are not the same. Orientation is one's private sexual behaviour life/private life. With integration into society, gender because it's a facet of social life, impacts the entire social group. Starts influencing interaction with others, requires public discourse and debate, very unlike sexaul orientation.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor on sports: Biological differences between men and women in sports. Endangers females in sports especially leaving out the idea of fairness and just speaking to physical issues. It's very much a recent issue. Dividing line is 2012 onset of social media, when adult transition mostly adult men transitioning, can't think of an individual prior to that of seeking participation in contact sports. If anything bio males would have preferred to avoid these kinds of activities the large-scale conversations FINDLAY objects. Says qualifications are insufficient for Cantor to comment on the participation of male-bodied people in sports. Bastow reads from ruling of the panel. FINDLAY: Has no qualification to comment on transwomen participating in sports. Bastow: Cantor is qualified to comment on hormonal differences and impacts and social impacts Panel is taking a moment to deliberate.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
why am I so interested in this topic asn speaking publicly? In 2008 my brother came out as trans in his 30s. Adult-Onset heterosexual male. no history of cross-sex identification. But history of other MH issues, including signs consistent with personality disorder and autism five 1/2 years ago I was alienated from my daughter by an affirming teacher and her mother (from whom I was divorced already for a number of years) My daughter has since medicalized, and recently changed from he/him pronouns to they/them.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
FINDLAY objects again about Cantor speaking on sports. Bastow moves Cantor on to regret from medicalized transitions and detransition Cantor: With adults, the changes that I've noticed with adults, the AGP pattern continues to be present. Things have become more ambiguous 18-20 years old not resembling adult features of transition the 18-20 are not representative of adult type and is a new phenomenon Brand new is Rapid Onset Type clustering of cases leading to the theory that a lot of adolescents cases fit the theory of social contagion... Outlines the susceptibility to social contagion... Socially Mediated Contagion online and occur in social clusters not in random isolated as in AGP and child onset
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor: if we are to use medical interventions we must rule out that this is a social contagion. Causation vs Correlation Is GD in ROGD the result of other mental health issues, or the other way around people are using threats of sui--de and threats of threats. Suic--de ideation and sui--de are different. Death, sudden event by self, is mostly male, middle-age. Suicidality is a cry for help, significant and important, but is not an early stage of what will lead to death. exaggerated emotional blackmail. emotional manipulation in an unhealthy social interaction. Giving in is not in the interest of the person. begets still more demands and doesn't held deal with the distress. People are taking such threats at face value and referring to sex-changing kids and lifesaving. No redux of rates of suicice and sewercidality after transition, they stay elevated after transitions
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor: best treatment is fulsome comprehensive mental health assessment and support PRIOR to any medical transition Note: Today FINDLAY is objecting on "leading questions" and unlike last week, she is being recognized by opposing counsel for fair objections. Bastow is rephrasing questions
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor: sexual minority stress is theoretically an interpretation for an increase in suicidality though it is not the only or the best explanation of possibilities. no controlled studies to give the most simple and straightforward explanation.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor: the kids who are most susceptible to this kind of social influence. Both GD and suic--lity are more likely caused by the same influences. ie social media Best course of action is psychotherapy
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor: the ethically appropriate course is to start with the intervention that causes the least amount of physical impact, ie psychotherapy, and is the most ethical intervention. We have no idea what is medically necessary... FINDLAY: objects to discussion of social media and social media influence. it looked like a member of the panel face-palmed and shook her head. FINDLAY: pushes her objection... note this is quite the non-sequitur, but trying to limit testimony. says he offers no expertise to speak to social media impacts. Bastow: not sure we need an expert to tell us Social Media has had an impact on the world we live in. Panel recesses for afternoon break
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Amy Hamm hearings resume: Back on the record with testimony of @JamesCantorPhD For the record: #IStandWithAmyHamm Panel rules Cantor is permitted to speak to role of social media in this case. FINDLAY was overruled. Bastow asks for "Minority Stress" definition Cantor: set of additional stressors over that of mainstream society and causes poorer mental health issues. It is a legit hypothesis at an individual level but no evidence in science is present or available for Adolescent onset of GD. We are not seeing stresses resolving after medicalization - label is used as a panacea explanation is it being used as an emotional blackmail or manipulation
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor: it is a violation of medical ethics when we cannot rule out the possibilities that MH improvements may be attributable to other causes besides treatment. We have a number of confounding factors (4) that may be giving indications that a hypothesis is is correct when it is not. Minority stress, once once starts controlling for other factors, don't have high quality studies to rule conclusions out. we can't make the conclusions that medical transition is the appropriate preventative for suicidal ideation due to minority stress. Bastow: very tolerant Sweden shows 19x higher suicide rates for post-transition people, lack of strong association between suicidality and transition. WPATH conceded that transition does not help to alleviate suicidality
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor on Borderline PD (personality disorder): has many different symptoms, based on a checklist #4 and #6 for diagnosis DSM #4 Repeated suicidal ideation and fantasies #6 unstable identity It's very easy for unstable identity to be confused with gender dysphoria. Very common for Suicidality in borderline PD. BPD is more common in females, teen onset, same sex ratio, same cohort, similar features to group that meets criteria that happens to match what people are seeing on social media wrt gender dysphoria.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
It's hard to imagine the panel might conclude that @preta_6 's public statements might be ruled inappropriate. @JamesCantorPhD raises so many evidenced-based inconsistencies in the facile narrative of the social media that the rainbow activists push so abusively that if the panel rules against Hamm, it really is evidence we're hopelessly corrupted by institutional capture.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor: defining trauma in it's actual physical impact terms to the diluted or eroded meaning of the terms like "harms." Histrionic filters use the most evocative language possible to describe situations and circumstances. People with minor or imagined slights might use these things as claims to trauma and harm. People's explanations are being taken at face value. Fashionable to not ask questions and to accept people's explanations at face value.
@ShannonBDouglas - Shannon B - Weekly Canadian Gender Wars Co-Host
Cantor: trigger warnings might be doing more harms than helping. After a generation of experimenting with these things, it appears that it trigger warnings concretize one's sense of victims Bastow pivots to misgendering, nice move Cantor: there is a subset of people driven by attention-seeking... challenging it (misgendering) or using the opportunity to attract attention as a expert to which others must defer to give attention to the seeker Cantor: Trigger Warnings and Misgendering taboos make the people more sensitive, moving people away from pro-social integration & more sensitive to slights Recommendations: Learn the skills to rise above appearances.

@sanjay_world - Sanjay "John"
Physicians, why is it so hard for you to accept that Med school is a Pharma sponsored brainwashing camp?
@_aussie17 - aussie17
🧵 1. I worked in Pharma for almost 20 years - mainly with the covid vaccine manufacturers as a commercial director. The vaccines are not safe and effective so I didn't take them. Please read the threads below to get an insider's view of how the Big Pharma machinery works.

@_aussie17 - aussie17
2. Here's how we calculate Net Patient Value (How much we can make per patient)

@_aussie17 - aussie17
6. How we target and segment doctors and change the behaviours of the ones that bring us the most $$$
@_aussie17 - aussie17
Read about my U-Turn here! All my contents are free - there are no paywalls. It's been a exactly a year since I started revealing info about Pharma practices. Education and awareness is key. Please share. https://www.aussie17.com/p/aussie17s-u-turn


@Prolotario1 - Ariel
-Brother Bilaal saw Will Smith having sexual intercourse with Duane Martin. -Melyssa Ford saw rapper Camron doing something sexual with a minor. -Jaguar Wright heard Patti Labelle had sex with all members of The Temptations while on tour. -Ron Savage saw African Bambatta doing sexually abusing little children. Listen, despite these allegations whether true/false when "The Machine" decides it no longer wants to keep the company of these Hollywood stars there is not a rumor, leak, or anything heard through the grapevine that will knock them down from their position. They are still useful for however much time they have left in Tinsel Town. P. Diddy is a prime example. 18 companies no longer associated with his brand. Hulu no longer wants to develop a show about P. Diddy. This is the nature of the beast. So I do not know why people assume anything else will suffice and have a equal affect in terms of exposure of certain activities they think will tank the careers that the industry as a whole will have once it decides you are dead weight or liability.

@kunley_drukpa - ɖʀʊӄքǟ ӄʊռʟɛʏ 🇧🇹🇹🇩
COMPILATION THREAD of Africans tweeting about fraudulently completing family members’ medical degrees After a now deleted tweet about Africans completing medical degrees for relatives went viral, some Africans began jokingly sharing their own experiences with degree fraud 🧵
















@kunley_drukpa - ɖʀʊӄքǟ ӄʊռʟɛʏ 🇧🇹🇹🇩
Reactions after ‘EDL Twitter’ finds the tweets and begins sharing them




















@kunley_drukpa - ɖʀʊӄքǟ ӄʊռʟɛʏ 🇧🇹🇹🇩
Influencer records video telling African Community off for tweets admitting to malpractice
@kunley_drukpa - ɖʀʊӄքǟ ӄʊռʟɛʏ 🇧🇹🇹🇩
According to the British General Medical Council, doctors who qualify outside of the UK are 3x more likely to be referred to them for malpractice vs UK trained doctors: https://www.gmc-uk.org/about/how-we-work/our-equality-diversity-and-inclusion-programme/our-targets-to-address-areas-of-inequality They apparently regard it is a disparate outcome to be remedied by DEI policy

@kunley_drukpa - ɖʀʊӄքǟ ӄʊռʟɛʏ 🇧🇹🇹🇩
In Ireland, of the 104 cases of medical misconduct from 2008-2023, 84% were non-Irish https://www.medicalcouncil.ie/Public-Information/Inquiry-Notifications/Fitness-to-Practise-Notifications/


@kunley_drukpa - ɖʀʊӄքǟ ӄʊռʟɛʏ 🇧🇹🇹🇩
Another useful compilation thread RE ongoing debates about Medical Malpractice https://t.co/MoaDJu02dO

@CompositeGuy_ - The Composite Guy
You can look up the doctors who have disciplinary hearings and find out who has been found guilty and who is cleared. The overwhelming majority of NHS doctors found guilty of malpractice are ethnic minorities https://mpts-uk.org/hearings-and-decisions/medical-practitioners-tribunals?page=1#decisionsTabLink https://t.co/B4upJ8ZBhR




@kunley_drukpa - ɖʀʊӄքǟ ӄʊռʟɛʏ 🇧🇹🇹🇩
Compilation of Afro Community TikToks discussing fraud and malpractice

@bourne_beth2345 - Beth Bourne
I wanted proof to show the world there was almost no stopping a trans-identified child from being medically "transitioned" at Kaiser Permanente once your child announced their trans 🏳️⚧️ identity. I wanted written records from the pediatricians in my town (Davis, CA) exactly what would be their protocol for medicalizing a child, and if there were any guardrails in place for parents like me who were not affirming. In order to do this, I pretended my younger child, my 15-year-old son, was interested in starting up on estrogen so he could present as female. Unlike his sister, my son had never experienced any distress over "gender" and wasn't likely to ever see this correspondence between his new pediatrician and me. Within 2 days, I received all the proof I needed to show how every pediatrician was completely captured by radical gender ideology and no child was safe under Kaiser's care. The responses get more shocking as I ask harder questions 🧵 @aboutKP@LeorSapir @wesyang @Miriam_Grossman @SwipeWright@shellenberger @benryanwriter @ErinFriday75490 @jessesingal@donoharm

@bourne_beth2345 - Beth Bourne
2/ Within 30 minutes, I hear back from my son's pediatrician. She says kids in Davis are often directly referred to the pediatric gender clinic, about an hour away in Oakland. I had already learned about the "Proud Clinic" with my daughter. This is a one-stop shop for transitioning kids with gender specialist counselors, fertility bank for storing sperm/eggs, and surgeons performing mastectomies "top surgery" on girls as young as 13.

@bourne_beth2345 - Beth Bourne
3/ My next question is an easy one. "Could you tell me how you make the determination that a patient is 🏳️⚧️transgender?" https://t.co/flHDpu7GPJ

@bourne_beth2345 - Beth Bourne
4/ Dr. Heidt quickly answers: "Usually it is the patient telling me how they identify. Some people feel strongly that they are male or female, no matter their gender at birth." So it's the child who is actually diagnosing himself or herself as transgender based on their feelings??!!

@bourne_beth2345 - Beth Bourne
5/ I ask the doctor if she might be willing to caution my son about the health risks of starting estrogen, feminizing hormone therapy, since he's only 15 years old. https://t.co/J5QCM8mRjT

@bourne_beth2345 - Beth Bourne
6/ Not only does Dr. Heidt skirt the issue of answering my question about the health risks associated with a 15-year old boy on cross-sex hormones, but she now responds with a message that now includes my ex-husband. She says: "I am here to speak with Nathan (my patient, not sure what they want to be called now) if they feel ready and want to talk with me and of course am happy to discuss with parents as well. "

@bourne_beth2345 - Beth Bourne
7/ I already knew the answer to this question since I had done my own undercover investigation where I pretended to be nonbinary, and my daughter's psychiatrist had warned me about a patient (13-year "nonbinary" girl) of hers that was prescribed testosterone on the first visit. But I still asked it: "Could you tell me the minimum number of sessions with a mental health evaluator before XXX (my son) could be prescribed estrogen? "

@bourne_beth2345 - Beth Bourne
8/ Dr. Heidt answers there is no "set number of sessions as every patient is different." She says not to worry, Kaiser isn't putting kids on wrong-sex hormones if they've only been thinking about it for a month or two as this would not be "consistent/persistent enough to meet the criteria." The criteria is 6 months. Insanity. 🚩🚩 She adds, "I know this can be very difficult as a parent but there are several excellent websites that you can check out." (all 3 are big TRA lobbying groups promoting the tran$ gender industry: TransParenting, Gender Spectrum, and Human Rights Campaign) 🏳️⚧️🏳️⚧️

@bourne_beth2345 - Beth Bourne
9/ Can children consent to being sterilized?? I decide to ask Dr. Heidt point-blank if she thinks my son is old enough at 15 to consent to taking life-altering drugs that could leave him sterilized. https://t.co/n3ecdUFOPr

@bourne_beth2345 - Beth Bourne
10/ My son's pediatrician acknowledges she can see in my son's records that his sister is "trans" and says parents need to consent. (What she doesn't say is that in California only one parent needs to consent and you will likely lose custody if you are the non-affirming parent holding the line.) 🚩🚩 She also says: "No one is going to force hormones on a child but rather offer support and affirmation for how a child is expressing themselves."

@bourne_beth2345 - Beth Bourne
11/ I pressed on and asked my son's pediatrician if there were any gender critical docs at Kaiser Davis. My friend in town had confided me in that there was a private group chat among her physician colleagues at Kaiser and a few docs had voiced their objection to being told to prescribe wrong-sex hormones to their patients - and instead were referring them to the new "gender affirming care" champion in the office, Dr. Yolanda Bakus. (The same doctor I met with for my undercover story where I pretended to be non-binary.) ...and I can't help myself with this question "Could you recommend another doctor at Kaiser Davis for my son who is not an activist?" 😂😂🤣

@bourne_beth2345 - Beth Bourne
12/12 And here it is, the proof. The Kaiser Permanente pediatricians will take no responsibility or blame for the destruction (cancer risks, sterility, irreversible genital surgeries, etc.) to your child. Dr. Heidt says: "As I mentioned in my first email, the primary care provider (whether it's a pediatrician or family medicine doctor) really has little oversight in this sort of situation." It's a big money $$$ generating pipeline for confused kids 🏳️⚧️🏳️⚧️ as Kaiser is an HMO, so both the insurer and the provider. All of the Kaiser members are paying the shared cost of putting these kids on wrong sex hormones, needing fertility banks, providing cosmetic double mastectomies for teen girls, etc. It's the most horrific medical scandal of modern times.


@DecentBackup - BackupDecentFiJC
👺MICHAL TOTCHANI: Hope you have a GREAT fucking attorney, c*nt. I regret to inform you, your crimes won’t be heard in Israeli courts, you fucking spy terrorist. (Btw, don’t bother leaving the country either.) 👺TOTCHANI: She’s a “former” IDF COMMANDER who worked in the ISRAELI PRIME MINISTER OFFICE as part of ISRAEL’S NATIONAL SECURITY COUNCIL. She was also the ASSISTANT to the HEAD OF LEGISLATION and LEGAL DEPARTMENT for ISRAELI MINISTRY OF JUSTICE. *These days she’s currently serving as… ✅TWITTERX Senior Policy Domain Specialist, Trust & Safety & Senior Policy Domain Expert *And before that, she was… ✅TIKTOK Product Policy Manager, Trust & Safety *But before THAT, and my FAVORITE of all… 👺JANUARY 2019: This bitch was at STANFORD UNIVERSITY working as a researcher in the STANFORD LAW SCHOOL “LAW AND POLICY LAB”, helping bake ANTI-WHITE BIAS into AI/ML PLATFORMS for future usage in HEALTHCARE SETTINGS. All under the guise of calibrating “ALGORITHMIC FAIRNESS” metrics into our fucking HEALTHCARE systems. “CURRENT ISSUES IN ARTIFICIAL INTELLIGENCE AND MACHINE LEARNING FOR HEALTHCARE” (Winter 2018-2019)




@DecentBackup - BackupDecentFiJC
STANFORD SMART HOSPITAL PROJECT 💥💥💥💥💥💥💥💥💥💥💥💥💥💥 “The Stanford School of Medicine and Computer Science departments have COLLABORATED to form the PARTNERSHIP IN AI-ASSISTED CARE (PAC), which leverages COMPUTER VISION and ML TECHNOLOGIES to solve PRESSING PROBLEMS in HEALTHCARE. The partnership is focused on FOUR CORE PROJECTS: 1. Hand Hygiene. 2. Senior Well-Being. 3. ICU Clinical Pathway Support. 4. Surgical Support.” Oh. I’m sure it gets even better from here.🤦🏻♂️ “AI/ML researchers are beginning to focus more on the task of creating algorithms that produce EQUITABLE OUTCOMES, an area often referred to as ALGORITHMIC FAIRNESS.” “IMPROVED CONTEXTUALIZED DECISION-MAKING …AI/ML DIAGNOSTIC TOOLS pull from LARGE DATA SETS, ideally with DIVERSE TRAINING SAMPLES. Physicians may not always have the same luxury to learn from diverse populations. For instance, DERMATOLOGISTS in MAJORITY WHITE COMMUNITIES may have TROUBLE DIAGNOSIS SKIN CANCER in PATIENTS OF COLOR. Whereas an AI DIAGNOSTIC TOOL could pool training data from OTHER LOCATIONS where the DATA SET is MORE REPRESENTATIVE.” Because that’s definitely how med school works, you retarded fucking fa***ts.🤦🏻♂️🤬 (CLIFFS: This is the part where they train their communist fucking AI/ML to overrule a PATIENT’S FUCKING PRIMARY HCP, should they determine a patient isn’t a “desirable” set of data for them.)




@DecentBackup - BackupDecentFiJC
“Even where doctors are PRESENT, they can be wrong, especially if they’ve had less advanced training.” Again, because that’s how med school works, you retarded fucking fa***ts.🤦🏻♂️🤬 Also, on a side note, WE have been RIGHT about literally EVERY FUCKING THING since COVID BEGAN, cunts. Meanwhile, you JEW “GLOBAL PUBLIC HEALTH” TERRORISTS have either been WRONG or just outright FUCKING LYING… while MURDERING PEOPLE. PS: For the foreseeable future, I’ll pass on the whole “DIAGNOSTIC AI/ML” version of the bastardized “peer reJew process” you fa***ts spent the last 6 years making a fucking mockery of, thank you very much. “From skin cancer classification to arrhythmia detection, HEALTHCARE AI/ML are INCREASINGLY OUTPERFORMING PHYSICIANS at certain tasks.” Define “outperforming” and be exactly specific.




@DecentBackup - BackupDecentFiJC
👺MICHAL TOTCHANI: She was also a “2019 FOUNDRY FELLOW” at the INTERNET LAW & POLICY FOUNDRY, serving as its COMMUNICATIONS DIRECTOR from 2019-2021. *TOTCHANI was in the same 2019 FOUNDRY FELLOW class with a buncha Jews/Mossad fa***ts from BOOZ ALLEN HAMILTON, NEW AMERICA, FACEBOOK, ORACLE and EQUAL JUSTICE WORKS (UJA/JDCA/Mossad), etc. *LEAH FARRAR was PRESIDENT of the 2019 FOUNDRY FELLOWS class. (Farrar, eh? Weird.) Imagine TF outta all THAT sports fans.😒




@DecentBackup - BackupDecentFiJC
More 2019 FOUNDRY FELLOWS.🖕 *There’s President Leah Farrar and Lena Ghamrawi from Booz Allen Hamilton. *LENA GHAMRAWI is also a POLICY COUNSEL at THE FUTURE OF PRIVACY FORUM and works on PRIVACY PROGRAMS for lots of FEDERAL AGENCIES and COMMERCIAL CLIENTS. Neat stuff, sports fans. Real neat. *ANDRES BASCUMBE works for MAXINE WATERS (Humpty Dumpty Institute/Jeffrey & Mark Epstein) and ANDREW MANLEY is an ATTORNEY ADVISOR for the FCC “MEDIA BUREAU”. *BEN WINTERS of the EQUAL JUSTICE WORKS “EPIC” program and CHARLES CHENG of ORACLE too.





@amuse - @amuse
DEI: Over 50% of medical students are accepted based on race and gender and not merit. Most white males who are more qualified and more likely to become the best doctors are excluded from US medical schools. https://t.co/HWUNFGTwAw

@Kevin_McKernan - Kevin McKernan
UPDATE! More people have weighed in on this including the authors of the Re-adenylation paper. They have been very transparent and helpful. The plasmid DNA is there. The 3’UTR sequence that matches the Fauci/Moderna synthetic constructs is shared sequence between the vaccines and points to a hole in our original assembly of the Moderna vaccines. Here is how we know. Thanks to @P_J_Buckhaults for suggesting this.

@Kevin_McKernan - Kevin McKernan
🔥Another Contaminant Found in the Moderna Vaccines. Did you consent to getting Moderna's HIV vaccine? Parts of it are in there. The recent Re-Adenylation paper has excellent sequence of not only the m1273 vaccine after application to mice.. but it also has the plasmid DNA https://t.co/tKBhuW65hb

@Kevin_McKernan - Kevin McKernan
If you map reads to the Moderna HIV constructs, you only get coverage over the ends of their HIV vaccines (I checked 4). You don’t get sequence coverage over the whole construct. That implies there are shared parts of the plasmids in these Moderna vaccines.
@Kevin_McKernan - Kevin McKernan
Why does our Moderna vaccine have a 60bp hole in it? We sequenced a bivalent vaccine. The assemblers, when faced with 2 conclusions average then into a consensus and this 60bp is jumbled as a result. BLAST is currently favoring the alignment to HIV vaccines over our Moderna C19 reference as it’s derived from monovalent sequence and more accurate.
@Kevin_McKernan - Kevin McKernan
There are now a few other sources of Moderna monovalent vaccine sequence that have teased this apart. One is in GitHub and I don’t know why BLAST isn’t prioritizing that BLAST hit over the HIV constructs. Still digging into that.
@Kevin_McKernan - Kevin McKernan
I want to thank @pakraw for being so open about their methods. They used a monovalent Moderna vaccine which will help clean up our bivalent reference sequence.
@Kevin_McKernan - Kevin McKernan
I could have submitted this for peer review. Maybe in 6 months this controversial topic would publish. Another 6 months for authors to reply and correct any issues. Instead, we have answers in 24 hours. The risk… the public gets to see the sausage of science. I prefer the later approach even if it can leave ‘egg on your face’ on occasion.
@Kevin_McKernan - Kevin McKernan
What did the public learn from this. 1)we now have 5 projects in the SRA where RNAseq is performed on vaccinated organisms and there is evidence of plasmid DNA in the patients. 2)Template switching is well documented by Moderna but this dataset doesn’t yet point to that. Maybe more digging will show it but these Fauci reads are better explained as a hole in our original Moderna reference (egg on face) 3)Moderna has many vaccines in development including HIV and Fauci is an author. This is a conflict if NIH is involved in granting them funds. $1.2B in C19vax royalty already flows into NIH.
@Kevin_McKernan - Kevin McKernan
When you get results that are as shocking as this it’s important to share with others and to hacksaw your hypothesis. I tried doing this by BLASTing these HIV sequences to all primers and probes listed in their supplement to see if anything else could explain the unexpected sequence. That was negative. The key was finding some homology in GitHub from Fires lab. It would be great if those reads were public as we’d have the plasmid-3’UTR junction better resolved.
@Kevin_McKernan - Kevin McKernan
This leads to a large culture question in science. Scientists use Retractions or correction as career ending moves. You can never be wrong. Publish or perish. This creates an insidious culture and explains why we don’t have a journal of negative results and witch hunt scientists over blurry bands on gels.
@Kevin_McKernan - Kevin McKernan
This cultures frowns on direct communication of results to the public without gatekeepers. This has enabled the peer review system to become completely captured and have better margins than google. Researchers give up their copyright, pay $5K per publication and review for free https://t.co/uQiEU5PYVn
@Kevin_McKernan - Kevin McKernan
The journals then become captive to their Pharma AD revenue and the editors decide what goes to review and what doesn’t. This is how we get Surgisphere, Proximal Origins, SSRI, Statins, Alzheimers Tau protein, Vioxx etc. We need a more transparent and decentralized approach
@Kevin_McKernan - Kevin McKernan
Some will claim you should delete your post if one iota of info is misleading. Not a chance. It’s important to see how conclusions were drawn and hypothesis nullified. Show your work. Don’t just spoon feed a conclusion, even if that at times bruises your ego.
@Kevin_McKernan - Kevin McKernan
90% of science is bruised ego and humility and the public only gets shown the times you are correct through peer review. This is unproductive. We have better communication tools now. What happened to Gutenberg? From chatGPT: Gutenberg’s printing press, developed around 1440–1450, was not immediately adopted or co-opted by the Church, but the Church did come to both utilize and regulate it relatively quickly. Initial Adoption: •Secular beginnings: Gutenberg’s first major work, the Gutenberg Bible (c. 1455), was a religious text, but it was produced independently by Gutenberg as a commercial venture—not under Church sponsorship. •Slow initial spread: The printing press spread gradually at first, mainly through private entrepreneurs and secular universities. Church Reaction: •Positive Utilization: Once its potential was recognized, the Catholic Church embraced the press to print Bibles, indulgences, and theological texts. Printed indulgences were among the earliest mass-produced items. •Censorship and Control: The Church also moved quickly to regulate printing. By the late 15th century, it began issuing indexes of prohibited books, particularly after the Reformation began (1517), when Martin Luther’s use of the press to spread dissent alarmed Church authorities. •Institutional involvement: Religious orders and bishops established printing presses, particularly in major religious centers like Rome and Cologne. Summary: The Church did not co-opt Gutenberg directly, but within a few decades it became both a major user and regulator of printing. Ironically, the same technology that helped spread official doctrine also enabled the Protestant Reformation, making control difficult.

@RepGregMurphy - Congressman Greg Murphy, M.D.
So troublesome to see so many young doctors complaining about how hard the job is. Your job is about taking care of patients. It’s called dedication. It’s called devotion. If you wanted an easy life, you should’ve chosen something else.

@catsscareme2021 - Jessica Rojas 🇺🇸💪
Imagine being 13… declared "brain-dead"… and waking up right before they cut you open for your organs. This isn’t a horror movie. It happened. A 13-year-old Alabama girl was set to become an organ donor. Her family was told she was gone forever. Machines were prepped, surgeons ready. Then-she moved. She opened her eyes. She LIVED. Doctors said she was "brain-dead." They were wrong. How many others have been silenced, buried, or cut open alive… all because of faulty tests and a rush to harvest? If you think hospitals don’t have financial incentives when it comes to organ donation, think again. Every single time a case like this emerges, officials say ‘protocol wasn’t followed.’ How many times do we need to hear that before we question the system itself?
@catsscareme2021 - Jessica Rojas 🇺🇸💪
How many people have to move, cry, or wake up right before organ harvesting before we call it what it is? This isn’t medicine- it’s a billion-dollar industry built on greed and deception.
@catsscareme2021 - Jessica Rojas 🇺🇸💪
@GenBelisarius That describes it perfectly, unfortunately 😕
@catsscareme2021 - Jessica Rojas 🇺🇸💪
@DrWojakMD I remember reading this on FB several years ago. It was my first wake up call regarding organ donation.. scary.
@catsscareme2021 - Jessica Rojas 🇺🇸💪
@SeanBFlanagan Too many! And they always call these "mistakes"
@catsscareme2021 - Jessica Rojas 🇺🇸💪
@fubots1 Smart! 🙏
@catsscareme2021 - Jessica Rojas 🇺🇸💪
@joe4deadcat It is! Did you ever watch the video with the Doctor who admits "brain death" is a lie?
@catsscareme2021 - Jessica Rojas 🇺🇸💪
@Kelly4Infowars I agree. The body will either reject the organs or it destroys their bodies because of the massive drugs they need to be on..
@catsscareme2021 - Jessica Rojas 🇺🇸💪
@boytzun You're very right ✅ it's like programmed robots who have been taught since childhood to obey, memorize, sit still and never question "authority" I get it.
@catsscareme2021 - Jessica Rojas 🇺🇸💪
@kristi10442 This is absolutely heartbreaking. I can’t imagine how that moment must stay with you. Thank you for sharing something so personal—your story matters, and I’m so sorry you had to go through that. 🙏
@catsscareme2021 - Jessica Rojas 🇺🇸💪
@suezq7369 Yes, they made a killing in many different ways during Covid, sadly.
@catsscareme2021 - Jessica Rojas 🇺🇸💪
@asamomma1 You're on to something.. Money, politics, and opaque policy can intersect dangerously in medicine.

@MrsDoubtFireSF - MrsDoubtFire🇺🇲 🫏🇺🇦 ⬜
In India, a five-year college undergrad can obtain MBBS to become a licensed practicing doctor without graduate school or formal residency. Would you trust an undergrad to be your #H1B doctor? India and Greg think you should! This is about India's H-1B economy, not healthcare.

@Vero_atLast - Vero
The medical school acceptance rate went like this for me in 2018. 4000 applied 375 interviewed for a class of 100. That's a 2.5% chance of getting accepted. 40% of my class was indian. I live in the south. The H1-B program should completely sunset. AAMC needs revolution

@AedmarSkyjarn - Aedmar Skýjárn
Anyone who incentivizes non-Whites over Whites for STEM education and employment should be herded into the sun with extreme prejudice. When this retarded boomer went to school and was hired, he didn't have to compete with endless third world trash because, at that time, universities and employers weren't forced to engage in judaized anti-White DEI practices.


@Cernovich - Cernovich
A friend of mine graduated medical school and didn’t match for his residency. I had no idea this happened. If they don’t match, they have to try again the next year. Sit in limbo. Rather than reform the residency system, we need more H-1B’s for private equity run hospitals? https://t.co/Cr7laHbsB5



@anonsynonymous6 - AnonSynonymous6
Why are there two sets of standards in US medicine? Those for US trained natural born citizens and those who are born outside the US? I was today years old when I learned in India people can go straight into "med school" from high school for a whopping 4.5 years. Then do a yr of clinicals and voila they are considered doctors. HOLY FUDDDGGGEEE To make it worse they are only expected to get 50% on all tests/clinical equivalents. DUDE To put it into perspective I had to have 2 years of pre req's before I ever entered nursing school. To get into nursing school you had to have a top 1-2% of the class GPA like mine...in my accelerated classes I had to get 100% on all nursing math tests. I had two chances or I could be kicked out of the nursing program...the standard hovered around 90% or better for everything else and this aligned with NCLEX standards at the time. This was pre AI, in an old fashioned classroom with a drill sergeant for an instructor breathing down your neck as you pencil in the answers... For your friggin ADN (Associates Degree in Nursing) you have 2 yrs pre Req's 2 yrs class and clinicals. 4 fuggin years to be an associates nurse in India they call that a doctor apparently BSN 2 yrs Pre Req's 4 yrs class and clinicals (combined/total)=6 years for a BSN all-in MSN/NP 2 yrs Pre Req's 6 yrs class and clinicals (combined/total)= 8 yrs all-in or if they go on for DNP 10 yrs all-in General MD: 8 years minimum just to get the degree (4 years undergrad/prerequisites + 4 years medical school). However, you cannot legally practice independently right out of medical school. You must complete a residency, which adds 3 to 4 years for fields like pediatrics or family medicine, making it 11 to 12 years all-in. General Surgeon: 13 years minimum. This requires the 8 years of school (undergrad + medical school) followed by a mandatory 5-year general surgery residency Specialty/Brain Surgeon (Neurosurgeon): 15 to 16 years minimum. Neurosurgery is the longest residency in the medical field. It requires the base 8 years of school plus a 7-year neurosurgery residency. If they want to specialize further in something like pediatric neurosurgery, they must complete an additional 1- to 2-year fellowship, pushing the total to 17 or 18 years I get there is supposed to be 'bridge' training when foreign nationals come here but what are we even doing...this is insane!!! @SecKennedy @JDVance @IngrahamAngle They are only expected to get 50% in India...like how is that even remotely fair to medical professionals in the US and how is that not a massive public health an safety issue??? I know for a fact bridge training is NOTHING like actual med school and nursing school in America when completing it comprehensively like we are expected to They are allowing these people to bypass standards even further on J-1 Visa as long as they serve in 'underserved areas' In other words we can't find anyone to work in rural America we don't care if you commit medical malpractice en masse we got lawyers for that they are poor and can't fight back anyway...@IngrahamAngle You have to cover this scandal in US medicine It's insane
@MyUnveiledTruth - Melissa
This is the Indian doctor who implanted a heart valve upside down in a child, and his education was completed in India. In India, a person only needs to earn 40% to pass, which is basically an ‘F’ in the U.S. Medical Degree: M.B.B.S., 1999, Madras Medical College, Chennai, India. Internship: General Surgery, Government General Hospital, Chennai, India (2001).


@JoshuaBradner - American as Trump
@MyUnveiledTruth @kate_p45 If you want to live, don’t go to the Indian doctor! https://t.co/CmRgvh5LUa

@_aussie17 - aussie17
1. New 🧵 Have you ever wondered why MOST doctors walk along the same lines when it comes to #MRNA shots, and VERY FEW doctors speak out against the narrative??? Read this thread to understand HOW Big Pharma GAGS your friendly doctor. https://t.co/nwp3ivGsC5

@TheOriginalSai - Sai
1. Thread: THE TRUTH ABOUT THE COVID-19 PANDEMIC FROM WITHIN THE NHS (EX DIRECTOR OF END OF LIFE CARE AT ONE OF THE LARGEST HOSPITAL TRUSTS IN THE UK) #NHS #Truth #Awareness #World #Freedom #Humanity #PowerToThePeople #Healthcare #COVID19 #CovidVaccine #VaccineDeath #Pandemic