reSee.it - Related Post Feed

@cidaqueiroz - Cida Queiroz⚡10 5 6 5
Denúncias do jornalista italiano Cesare Sacchetti! As autópsias de Bergamo: "o principal problema não era o #VirusChines Vou traduzir somente os pontos mais importantes. O texto é longo. ⬇ https://lacrunadellago.net/2020/04/25/le-autopsie-di-bergamoil-problema-principale-non-era-il-coronavirus/

@cidaqueiroz - Cida Queiroz⚡10 5 6 5
O médico Giampaolo Palma, cardiologista com grande experiência, trabalhando atualmente no centro especializado para doenças cardiovasculares em Salerno, ⬇
@cidaqueiroz - Cida Queiroz⚡10 5 6 5
explicou minuciosamente quais podem ter sido as reais causas da morte dos pacientes do Covid. As mortes ocorridas em Bergamo não seriam em consequência da pneumonia intersticial, mas resultado de microtromboses venosas. ⬇
@cidaqueiroz - Cida Queiroz⚡10 5 6 5
Após as execuções das autópsias de 50 cadáveres no Hospital Papa João XXIII e outras 20 no Hospital Sacco de Milão, a comunidade médico-científica parece haver chegado a esta conclusão que muda completamente a narrativa feita até agora. ⬇
@cidaqueiroz - Cida Queiroz⚡10 5 6 5
O coronavirus não atacca primeiro os pulmões, mas atinge sobretudo os vasos sanguíneos, impedindo o regular afluxo de sangue. Seria uma doença inflamatória vascular sistêmica. ⬇
@cidaqueiroz - Cida Queiroz⚡10 5 6 5
E o doutor Palma explica como o virus ataca o organismo de uma pessoa. “Senhores, Covid-19 danifica primeiro os vasos, o sistema cardiovascular, e só depois chega aos pulmões! São as microtromboses venosas, não a pneumonia a determinar a fatalidade!" ⬇
@cidaqueiroz - Cida Queiroz⚡10 5 6 5
Logo, se o Covid atinge primeiro os vasos e o sistema circulatório, a dedução natural é que seja inútil ventilar artificialmente os pacientes, isso para não dizer prejudicial, a partir do momento que os pulmões não estão recebendo sangue suficiente. ⬇
@cidaqueiroz - Cida Queiroz⚡10 5 6 5
“Se ventile um pulmão onde o sangue não chega, não adianta! De fato, morrem 9 pacientes a cada 10!" Os respiradores artificiais não resolveram o problema, ao contrário o agravaram. Confirmações neste sentido estão chegando também dos Estados Unidos. ⬇
@cidaqueiroz - Cida Queiroz⚡10 5 6 5
A emergência do coronavirus serviu para instaurar uma ditadura. Então, se o problema de toda esta emergência foram o diagnóstico e o tratamento errados, o perigo do vírus desaparece. ⬇
@cidaqueiroz - Cida Queiroz⚡10 5 6 5
Toda a mídia e o governo, com suas várias e caras forças-tarefa, logo associaram as causas das mortes ao coronavírus, sem nem ao menos saber o que realmente tinha acontecido. Basta pensar no lúgubre espetáculo dos caminhões militares em Bergamo que transportavam os mortos. ⬇
@cidaqueiroz - Cida Queiroz⚡10 5 6 5
Amigos, compartilhem ao máximo essa notícia. É de utilidade pública‼ Sr Presidente @jairbolsonaro @TeichNelson @minsaude Sob o ponto de vista médico é urgente verificar as descobertas do médico italiano.
@cidaqueiroz - Cida Queiroz⚡10 5 6 5
Sob o ponto de vista político, continuo afirmando que a quarentena é uma farsa. Implantar uma ditadura, promover o caos, criação de caixa 2, derrubada do Presidente, é o objetivo dos governadores brasileiros.

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
Associazione francese delle vittime dei VACClNl: "Cerchiamo questa signora per una pubblicazione su Lancet sugli effetti collaterali. Il governo dovrebbe reagire entro 24 ore dalla pubblicazione."😂 La storia della frode di Lancet sull'lDROSSlCLOROCHlNA. Thread



@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
2. Lancet il 22 maggio 2020 pubblicò lo studio che "ha dimostrato che con l'lDROSSlCLOROCHlNA aumentava la mortalità", spingendo l'OMS a bandirla. Coautore dello studio è il Dr. Sapan Desai, che ha fornito i dati della sua società medica Surgisphere. https://web.archive.org/web/20200522141513/https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31180-6/fulltext

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
3. Surgisphere del Dr. Sapan Desai l'lDROSSlCLOROCHlNA ha anche la filiale Quartz Clinical. Surgisphere afferma di aver ricevuto i dati da ben 1.200 ospedali, ma senza fornire le fonti. Doveva bastare questo dato assurdo per far allarmare Lancet, ma se ne fregano e lo pubblicano.

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
4. Il 28 maggio 2020, oltre 200 ricercatori e medici tra cui il Prof. Didier Rault, scrivono a Lancet affermando che "sia il numero di casi e decessi che la raccolta di dati sembrano improbabili". Il "fact-checker" 🤡 francese prova subito a diffamare Rault scrivendo a Lancet.

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
5. Il 5 giugno i coautori Mandeep Mehra, Frank Ruschitzka e Amit Patel, si accorgono "improvvisamente" che i dati forniti da Surgisphere dal Dr. Sapan Desai, sono probabilmente falsi e decidono così di ritirare lo "studio". https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31180-6/fulltext https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31324-6/fulltext
@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
6. Incredibilmente, neanche Amit Patel si sarebbe accorto che i dati di Surgisphere del Dr. Sapan Desai erano probabilmente falsi, nonostante risulterebbero sposati (tra loro).


@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
7. Eccoci alla signora della foto iniziale, Ariane Anderson, responsabile di Surgisphere del Dr. Sapan Desai e direttrice alle vendite della sua filiale Quartz Clinical (vedi tweet 3), con la passione della fotografia "artistica". https://www.modelmayhem.com/portfolio/805464/viewall promotelive.com/talent-profile…



@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
8. Ariane Anderson, responsabile di Surgisphere del Dr. Sapan Desai, fonte dei dati FALSI per lo studio FALSO contro l'lDROSSlCLOROCHlNA pubblicato da Lancet e poi ritirato, quando ormai si era consolidata la FRODE scientifica nel "consenso-scientifico™". Punto di non ritorno. https://t.co/FpH3G5GeSU


@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
9. L'inchiesta del Dr. James Todaro sulla FRODE scientifica di Lancet contro l'lVERMECTlN: "La disinformazione è negativa. La disinformazione in medicina è peggiore. La disinformazione proveniente da una prestigiosa rivista medica è la peggiore." https://archive.is/2020.06.03-202746/https://www.medicineuncensored.com/a-study-out-of-thin-air

@Jikkyleaks - Jikkyleaks 🐭
HOLY CRAP This is the data for midazolam prescribing from the UKs official prescriber database I have no words. #3tablets #democide @chrismartenson @Fynnderella1 @EWoodhouse7 @jjcouey https://openprescribing.net/analyse/#org=regional_team&numIds=0408020W0,1501041T0,0408020V0,0401010Q0&denom=nothing&selectedTab=chart…

@Jikkyleaks - Jikkyleaks 🐭
@chrismartenson @Fynnderella1 @EWoodhouse7 @jjcouey What needs to happen now is an audit needs to be undertaken of deaths in care homes where midazolam usage was high. If the patients that died were given midazolam instead of antibiotics in March - May 2022, criminal charges must be laid. But who created the policy?
@Jikkyleaks - Jikkyleaks 🐭
@chrismartenson @Fynnderella1 @EWoodhouse7 @jjcouey Just a note that the chart above is created from the GP prescriber database. Therefore it should not be impacted by any increase in ICU admission or specific use for ventilation. This looks to be solely for use in nursing homes and at home. Harold Shipman style.

@Jikkyleaks - Jikkyleaks 🐭
Bad Cheese 🧀🧀🧀 A point of note - the spike in midazolam prescription (on this *GP* database) was driven almost entirely by injectable 10mg/2ml doses (1501041T0). This was not the anxiolytic oral form. It's a euthanasia injection. https://openprescribing.net/analyse/#org=regional_team&numIds=1501041T0AAAAAA&denom=nothing&selectedTab=chart

@Jikkyleaks - Jikkyleaks 🐭
For those claiming that these drugs were being used for ventilating people in hospital, a reminder that this is the GP prescribing database. An example - prescriptions for propofol (only used in hospital) - zero

@Jikkyleaks - Jikkyleaks 🐭
This is damning - NSW health. How the hell can you justify an "anticipated end of life care" for a pneumonia? Seriously - what is wrong with you people? (archived) https://www.health.nsw.gov.au/Infectious/covid-19/communities-of-practice/Pages/guide-medication-prescribing.aspx
@Jikkyleaks - Jikkyleaks 🐭
Archive https://archive.is/L6fQ3
@Jikkyleaks - Jikkyleaks 🐭


@Jikkyleaks - Jikkyleaks 🐭
@Jikkyleaks - Jikkyleaks 🐭
BOMBSHELL: For those doubting Matt Hancock and @drlukeevans desperation to euthanise elderly in care homes in April 2020. ▶️10% immediate drop in care home occupancy. ▶️55,000 deaths. ▶️11-sigma Harold Shipman was a warm up. #Gerigate @MaajidNawaz https://www.statista.com/statistics/1231777/care-home-occupancy-in-the-uk/


@PWestoff - Paul Weston
@IsabelOakeshott The data doesn't lie, Ms Oakeshott. The data isn't "crazy." The ONLY wave of excess deaths in 2020 occurred over just 6-8 weeks amongst the old and ill in care homes. This coincided with large scale prescriptions of Midazolam. See below. What are your thoughts on this reality? https://t.co/PjMCqVSUfw



@madelynrogers - Emma Peel UK☯️
Remember the FEAR around the world when Italy was on every MSM news outlet, covid February 2020. Photos of coffins were from a ship sinking in 2013. Yes there were elderly deaths, caused by Untreated severe flu, patients were 'made comfortable' with #midazolam & same in the UK





@matt7gh - Matteo Galante 🇷🇺 🐭
L’IDROSSICLOROCHINA FUNZIONA (thread) 1/ L’#idrossiclorochina è un farmaco in uso da decine di anni. Il suo utilizzo contro il #Covid fu bloccato a causa di uno studio FALSO uscito sul #Lancet. Però l’idrossiclorochina funziona contro il #COVID19 👇
@matt7gh - Matteo Galante 🇷🇺 🐭
2/ In questo studio, che DIMOSTRA che la #terapiadomicilare guarisce dal #COVID19, si legge che i #medici hanno usato fra i tanti farmaci anche l’#idrossiclorochina https://www.mdpi.com/2077-0383/11/20/6138


@matt7gh - Matteo Galante 🇷🇺 🐭
3/ Persino #Burioni aveva partecipato ad uno studio che dimostrava l’efficacia dell’#idrossiclorochina contro il #COVID19 (in vitro).
@matt7gh - Matteo Galante 🇷🇺 🐭
4/ Infine questa testimonianza da #presadiretta DIMOSTRA che l’#idrossiclorochina veniva usata contro il #COVID19 a Bologna nel 2020 e FUNZIONAVA
@matt7gh - Matteo Galante 🇷🇺 🐭
5/ E non c’è nemmeno bisogno di scomodare il discusso scienziato Didier Raoult che #troll #provax e disinformatori prezzolati cercano invano di screditare, per attaccare l'#idrossiclorochina e quindi le cure per il #COVID19
@matt7gh - Matteo Galante 🇷🇺 🐭
6/ Studio che dimostra la sicurezza dell'#idrossiclorochina nel trattamento del #Covid e quindi smentisce anche i peracottari #provax sulla pericolosità di questo #farmaco Grazie a @Lancillotto810 per la scoperta https://www.mdpi.com/1648-9144/59/5/863


@CanariesBlue - Blue Canaries (Publius)
1) MIDAZOLAM & COVID - In the US, Midazolam is one of the drugs used in lethal injections for those who receive the death penalty in some states. Many in the UK claim that the US death row killer, Midalozam was used to EUTHANIZE many of their elderly. I dive into this.




@CanariesBlue - Blue Canaries (Publius)
2) "Section 2 of the 2019 World Health Organization Model List of Essential Medicines includes opioid analgesics formulations commonly used for the control of pain and respiratory distress, as well as sedative and anxiolytic substances such as midazolam and diazepam." 4/2020




@CanariesBlue - Blue Canaries (Publius)
3) The use of Midazolam in combination with other drugs is discussed, but for what purpose? "A patient who is fighting for breath can best be helped using medications that reduce the effort required to breathe and alleviate the fear of dying" https://tidsskriftet.no/en/2020/05/debatt/relieving-sensation-suffocation-patients-dying-covid-19

@CanariesBlue - Blue Canaries (Publius)
4) Please read through the Briefing Notes. Those who are in Respiratory Distress and experiencing Restlessness and Anxiety and Acute Agitation and Delirium.



@CanariesBlue - Blue Canaries (Publius)
5) According to protocols, it does not appear that Midazolam was used as a life saving measure, but yet as an end of life decision. The same punishment that is giving to those on death row in some US states. Conveniently, it would be classified as a COVID death.
@CanariesBlue - Blue Canaries (Publius)
6) Is my comparison to the lethal death penalty dose a fair comparison? If you consider the fact that Midazolam should be carefully used in the ELDERLY under normal circumstances, what kind of precautions should be used in an ELDERLY person with a respiratory illness?




@CanariesBlue - Blue Canaries (Publius)
7) "Seven studies, documenting the care of 493 patients met the inclusion criteria. Approximately two thirds of patients required a continuous subcutaneous infusion with median doses of 15 mg morphine and 10 mg midazolam in the last 24 h of life." https://journals.sagepub.com/doi/full/10.1177/02692163211013255
@CanariesBlue - Blue Canaries (Publius)
8) This discusses Provider Level Availability Issues and how they were working to increase the national stockpile. They EVEN asked Governors of US States that use these drugs in the death penalty to RELEASE their stockpiled drugs. 👈 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7204700/


@CanariesBlue - Blue Canaries (Publius)
9) In 2018 - there were 2 procurements for the National Stockpile of Midazolam - this one in June which was for a continuation of an earlier contract.




@CanariesBlue - Blue Canaries (Publius)
10) This Compounded Pharmaceuticals procurement was in April 2018.


@CanariesBlue - Blue Canaries (Publius)
11) Early on, I was tracking COVID deaths in my area. Many of the early deaths were in nursing homes. Matter of fact, it was two-thirds of early COVID deaths were those in the nursing homes.
@CanariesBlue - Blue Canaries (Publius)
#NursingHome #Austin #COVID19 "The nursing home population in particular is shockingly vulnerable," Dean Johnston told Austin City Council members Tuesday. He said two-thirds of the area’s COVID-19 deaths were among nursing home patients and staff. https://www.kut.org/post/911-calls-illustrate-covid-19s-spread-austin-nursing-homes

@CanariesBlue - Blue Canaries (Publius)
12) The numbers change depending on area, but this AARP article claimed that residents and staff of long-term care facilities were 7 times as likely to die of COVID-19. (2/15/2021)



@CanariesBlue - Blue Canaries (Publius)
13) We all know that officials claimed there was no treatment for COVID, but there was a death plan (identified earlier) for SOME people with COVID. They had a national stockpile of Midalozam as well as Midalozam in the Compounded Form. Who decides what is in the stockpile?
@CanariesBlue - Blue Canaries (Publius)
14) Project BioShield was established under Pres. Bush and it is responsible for the national stockpiles. This program allows the US GOV to purchase drugs and vaccines to put into a national stockpile in the event of a national emergency. https://georgewbush-whitehouse.archives.gov/infocus/bioshield/index.html

@CanariesBlue - Blue Canaries (Publius)
15) The concerning thing now is that they are replenishing Milazopan. This time they are procuring a needle-free version. You know so you won't have to worry about those silly needle marks when you are on your deathbed.
@CanariesBlue - Blue Canaries (Publius)
16) As part of this contract, BARDA awarded $60 million to Crossject for an initial order of ZENEO® Midazolam as soon as the product is authorized by the FDA. BARDA also has an option for the acquisition of additional units, up to $59 million... https://www.globenewswire.com/news-release/2022/06/18/2464968/0/en/CROSSJECT-Agreement-with-BARDA-on-ZENEO-Midazolam.html
@CanariesBlue - Blue Canaries (Publius)
17) This project is supported in whole or in part with federal funds from the U.S. Dept of Health and Human Services, Office of the Asst Secretary for Preparedness and Response, Biomedical Advanced Research and Development Authority (BARDA), under Contract No. 75A50122C00031. https://t.co/0YSemPdONz

@CanariesBlue - Blue Canaries (Publius)
18) This mean that you, as a taxpayer, have already paid for needle-free death shot. Have we already been sentenced to death, is the question? https://t.co/ksZIr9SDcX

@ng16322 - NG16322
#midazolam Matt Hancock authorised NICE Guideline NG163 to euthanise elderly in NHS UK. *Special Considerations* respiratory problems? - give them more midazolam until they DIE #NG163 #CrimesAgainstHumanity #Sunak #ToryBrokenBritain #ToryCriminalsUnfitToGovern #Nuremberg2 #NHS


@Red_Pill_Report - On m'appelle 404
Le décret ( signé par Olivier Véran et Edouard Philippe ) sur l'utilisation du Rivotril en Ehpad a permis , par le raccourcissement de la durée de vie de nos aînés , de créer la première vague de faux Covid en France . Pierre Chaillot , statisticien https://t.co/Z9plXDVLhT
@gigirmc - Jean-Jacques Robin ن
Un rapport de l’assemblée nationale fait état de la moitié des décès de la 1er année de Covid dans les Ephad ! Ce qui diminue d’autant la soit disant vague de mortalité ! Les Ephad avaient tout simplement été oubliées par les ARS dans leur plan anti Covid! Le rattrapage de cet oubli scandaleux a été fait à coup de dose de Rivotril qui un dépresseur respiratoire et qui a donc emporté, dans le silence des Ephad interdites au publics, nos anciens ! Qui sera jugé pour cette forme d’euthanasie!

@Inversionism - Inversionism
COVID-19 Respiratory Management and Critical Care Reference Guide for 2020 - Ventilators, Ketamine, Fentanyl, Propofol, Midazolam, and other drugs. Have you ever wondered what the full medical procedure guidelines were for putting someone on a ventilator during the COVID pandemic in 2020? Look no further, as I have finally located the document in my archives that details the ENTIRE process, what drugs they give, and how they manage patients on the ventilator with various drugs such as fentanyl, ketamine, and the well known Midazolam, which was often lethal. This is what the complete capture of medicine by pharmaceutical companies looks like. None of this has the wellbeing of the patient in mind. It's just pharma and medical companies trying to cram in as many drugs and procedures as possible to milk you and the insurance company for every penny, and to keep you in the hospital for as long as possible. Even worse, if this process kills you, they get paid an additional amount from the government via the CARES act. This is why mortality was so high during the beginning of COVID in 2020. Combine all these drugs being used to put you to sleep + ventilation + remdesivir = euthanasia. Image 1: COVID-19 AIRWAY MANAGEMENT ALGORITHM Image 2/3: UUED COVID-19 Intubation Plan Image 4: CRITICAL CARE IN COVID-19





@JacquiDeevoy1 - Jacqui Deevoy
1/2 This morning, I sent this email to 30 mainstream editors and news-desks. I’ll let you know how they respond. “Dear all, As you may remember, for the last three years, I’ve been investigating the euthanasia that’s been blatantly carried out in U.K. care homes and hospitals. I’ve pitched stories to you on this subject regularly during this time. Most of you have ignored those pitches. In 2021, I met with Sam Greenhill (news editor at the Daily Mail and cc’ed here) and Stephen Adams (the then medical editor at the Mail on Sunday). Both wanted to run the story but later changed their minds. They decided there wasn’t enough evidence. At the time, I had 16 people willing to speak out. Two years down the line, I have 87, most with incontrovertible evidence - evidence that includes medical records, drug charts and recorded phone calls. On Saturday, the story finally hit the mainstream. Neil Oliver of GB News finally (after much encouragement from myself and the man who originally came to me with the story) presented a show focusing on this shocking topic. Here’s a link to it: https://youtube.com/watch?v=o3nsZiiT4YU… For your reference, here’s the pitch I sentto 28 editors in 2021 and updated to include a higher number of case studies and information about a documentary I made: ‘Euthanasia is being used as a medical protocol in UK hospitals and care homes’ Extensive research reveals that the Liverpool Care Pathway, which was abolished in 2014 after being deemed inhumane, was brought back in at the start of the pandemic in early 2020 (NICE guideline NG163) and has since been used in hospitals and care homes across the UK. Evidence includes the following: · A House Of Commons document (a Hansard script) detailing a conversation between Health Secretary Matt Hancock and Conservative MP Dr. Luke Evans, during which they discuss the use of certain medications - namely the benzodiazepine Midazolam and the opioid morphine- to give Covid patients a “good death”. A good death is medical terminology for euthanasia. (‘Euthanasia means ‘a good death’ in Greek.) · A video of the above conversation. · Confirmation of Hancock ordering two years’ worth of a sedative called Midazolam from Accord, a French supplier. The order was made in March 2020. It was claimed at the time that the drug was for the treatment of Covid patients. Midazolam suppresses the respiratory system. Covid is a respiratory disease. Midazolam is used as an execution drug in the US. A two-year supply was ordered and was used within nine months. · Quotes from doctors, medical researchers, pathologists and pharmacists confirming what Midazolam is, what it's for and how it should and shouldn’t be used. Evidence from the BNF that benzodiazepines and opioids should never be used concomitantly. · Paperwork and links showing the LCP protocol was reintroduced in early 2020. This time around, it wasn’t called the Liverpool Care Pathway - it was called NG163 - but the protocol was identical: the use of a cocktail of drugs (a benzodiazepine and an opioid, usually Midazolam and morphine), along with a withdrawal of food and water and necessary medications, leading to the hastened and untimely death of the patient. · Documents (medical records and drug charts) showing the dosage of Midazolam and morphine given to Covid patients and showing how breathlessness in patients is to be managed using these drugs. · Information from anonymous insiders - including lawyers, doctors, care workers and nurses, who’ve seen this abominable practice happening first hand. · A video made by Manchester mayoral candidate Michael Elston, outlining what he knows to be happening with regards to the killing and culling of the elderly using Midazolam.
@JacquiDeevoy1 - Jacqui Deevoy
2/2 · 87 case studies who are willing to speak to the Press about their loved ones’ deaths being hastened in hospitals and care homes. One case is historic and occurred whilst the LCP was still in place; the rest have happened in the last three years; three are ‘near miss’ stories - one, when a woman who had nothing wrong with her was put on end of life treatment only to be rescued by her niece at the last minute; a woman who rescued her sister and a man who survived the LCP 13 years ago. Many people believe it’s acceptable for the sick and elderly to be given a pharmaceutical “helping hand” when they’re in - what’s deemed to be - the final stages of their lives. Few seem to realise that euthanasia (in any form – voluntary or involuntary) is illegal in the UK. If a person is found to be involved in euthanasia, they risk a life sentence. Those found guilty and charged with “assisted suicide” can get 14 years in prison. The problem my case studies have is that NONE of their loved ones were terminally ill and many of them were under 70. The normalisation of euthanasia has been occurring for years. In 2020, the then health secretary Matt Hancock started to push for the legalisation of assisted suicide. In the last three years, the Assisted Dying bill has been debated in parliament many times. In the meantime, thousands are being euthanised every day. It’s been reported that around 130,000 people are euthanised in hospitals, hospices and care homes every year. Many medics know this is happening but turn a blind eye. In 2021, due to the papers refusing to run any stories on this subject, I made a documentary: ‘A Good Death?’ It’s been seen by millions since it premiered and has woken up many people to what went on behind the locked doors of hospitals and care homes during the pandemic. Here’s a direct link to the film: https://www.ickonic.com/Watch/1163 In recent months, one broadsheet editor has approached me, wanting to hear more, but they’re moving very slowly and haven’t published anything yet. If you’re interested in being the first paper to break this story, I’d be happy to help you. (As some of you will know, I’ve been a freelance journalist for 38 years and have written hundreds of articles for the national newspapers.) Since I first sent this pitch, I’ve written many articles for non-mainstream news outlets and have been interviewed for internet radio and TV shows on at least 50 occasions. I hope now that, in the light of the GB News report, you’re interested in my work and that you’ll see how important it is to get this story out there. Your readers need to know the truth. Looking forward to hearing from you. Regards, Jacqui Deevoy
@JacquiDeevoy1 - Jacqui Deevoy
I’ve sent this to 30 mainstream newspaper editors. Reckon they’ll publish it? Hancock’s deadly Covid protocol was slammed by doctors in 2020… but he implemented it anyway By Jacqui Deevoy When former health secretary Matt Hancock first came up with NG163 (the Covid protocol reminiscent of the abolished Liverpool Care Pathway that was used to treat the elderly and those presenting with respiratory issues in hospitals and care homes) in early 2020, he was quickly presented with the advice of nine doctors and two professors, all of whom were familiar with end of life care procedure. After studying it, they said they were “concerned that uncritical use of NG163 may create unintended risks for people with suspected or actual COVID-19 infection” and suggested that it shouldn’t be implemented. The new guideline replaced NG31, which detailed how to deal with people dying of cancer. The doctors pointed out that, with regards to the old guideline, the evidence base was so poor that specific dosages were not recommended. They seemed confused by the fact that dosages recommended in NG163 were so specific. In a letter, published on April 20th 2020, the eminent experts, led by Professor Emeritus Sam H. Ahmedzai, point out that “while NG163 states ‘Note that symptoms can change, and patients can deteriorate rapidly in a few hours or less’, there is no counterpoint that most patients without the preconditions above will eventually recover.” They also state that, while there was plenty of detail on dosing up Covid patients with powerful medications, there’s no advice on monitoring the patients nor on weaning them off the drugs. Could that be because there was never any intention of weaning them off? Another major concern of the panel was the fact that NG163 states: “Sedation and opioid use should not be withheld because of a fear of causing respiratory depression.” This is probably the most frightening line ever to be written into a NICE guideline as it’s telling nurses not to be put off giving the prescribed drugs due to a fear that the patient’s breathing will dramatically slow down. They’re being told to disregard any concerns and administer the drugs anyway. Doctors prescribing the meds - and many of the nurses giving them - KNOW that using Midazolam and morphine together will slow down breathing (to the point of death if it’s administered continuously via a syringe driver) but this very clear instruction is telling them not to worry about that! How many medics administered this killer cocktail of ‘end of life drugs’ to patients, not all of whom were presenting with respiratory symptoms - or, in some cases, appearing to have nothing more than a positive result from a non-diagnostic, not fit-for-purpose PCR test - knowing it was going to kill them? Some doctors and nurses have since admitted wondering about the potentially lethal effect of this combination of benzodiazepines and opioids and knew that the doses they were giving were way too high (something else that was a point of concern in the letter), but very few spoke out and the vast majority just continued to follow orders. Sadly, as we know from the Nuremberg Trials, the excuse of “just following orders” does not stand up in court. (And, whether they knew the dangers of what they were doing or not, court is where many of these obedient ‘angels of death’ will end up.) (More to follow in comments below.)

@EusebeRioche - Complotisme à l'ancienne
La notice est claire: pour tuer un vieux, mettez-le sous Midazolam ! N'utilisez jamais le Midazolam chez les + de 60 ans, sinon: - arrêt cardiaque ; - arrêt respiratoire. Vous voulez une épidémie de «cas graves» ? Multipliez par 2400 sa conso mensuelle. …https://base-donnees-publique.medicaments.gouv.fr/affichageDoc.php?specid=63020895&typedoc=N…





@LazzaroDelPrete - Lazar Kaganovich
Thread 1. Partiamo da un case history. In GB si è osservato un dato. Il vaccino per il morbillo, che funziona egregiamente, non immiunizza del tutto. Necessita richiami. Quindi, la tua immunità (ovviamente a contagio avvenuto, perché NESSUN VACCINO impedisce il contagio) non
@redazioneiene - Le Iene
Caro Prof. Bassetti, non siamo medici (come lei reclama) ma non siamo stupidi e in questi mesi abbiamo parlato con tanti medici che non la pensano come lei. Ha passato due anni a sostenere che il plasma iperimmune non funzionava, e adesso deve ricredersi. E fortunatamente dichiara (cosa che non ha mai fatto prima) che se usato entro i primi 5 giorni “può avere un ruolo”. Anche gli antibiotici se non li si usa per tempo e nel giusto modo non servono a nulla. Adesso lei puntualizza: “Ma attenzione, il plasma iperimmune non è, come viene detto, un farmaco a costo zero”. Caro professore, non c’è niente che costa zero. Sicuramente costa 10 volte meno di una cura monoclonale prodotta da una multinazionale farmaceutica. Il plasma iperimmune è stato donato dalle persone guarite, che hanno prodotto anticorpi che sono serviti a guarire altre persone. Il costo di questo procedimento è 80/100 euro a sacca. Per una cura completa servono mediamente 4 sacche. Il Prof. Bassetti dice: “Ci vogliono donatori, bisogna organizzare e non è così semplice”. Anche per andare a comprare un’aspirina in farmacia bisogna organizzarsi. Lasci fare ai medici dell’ospedale pubblico di Padova, che si sono organizzati benissimo e che hanno distribuito plasma iperimmune a 1500 esseri umani, non andando contro la scienza, curando un sacco di persone e disobbedendo a chi in questi anni di covid li ha combattuti da giornali e reti televisive unificate. Fortunatamente oggi il virus sembra essere molto meno aggressivo, ma alla prossima pandemia, che nessuno si augura, questo sistema di cura dovrà esser preso in considerazione più seriamente. Lascio di seguito i link degli articoli sul funzionamento del sangue iperimmune pubblicati dalle più importanti riviste scientifiche https://www.medrxiv.org/content/10.1101/2022.05.24.22275478v3 https://www.nejm.org/doi/full/10.1056/NEJMoa2209502 https://onlinelibrary.wiley.com/doi/10.1111/vox.13498 Non è mai troppo tardi recitava il maestro Alberto Manzi. Speriamo.

@LazzaroDelPrete - Lazar Kaganovich
2. È assoluta, come sarebbe se tu fossi un guarito. Problema: da bambini sviluppa sintomi esantematici, da adulti su arriva all'encefalite, e ha spesso esiti letali. Risultato? Ritardando l'eventuale immunizzazione, ed avendo immunità non assoluta, le probabilità di
@LazzaroDelPrete - Lazar Kaganovich
3. Prendere il morbillo si sono spostate verso l'età adulta. Quindi, paradossalmente, la campagna vaccinale ha AUMENTATO la letalita. Letalita = morti / casi. Quindi? La sanità ha bisogno di organizzazione e management su larga scala, cosa che non prevede la lettura
@LazzaroDelPrete - Lazar Kaganovich
4. Di open o di blog sgrammaticati di bugiardi delatori. Altro esempio: monkey pox. Si vaccina, e NESSUN apparato di comunicazione mainstream ha parlato di DPI, cioè il benedetto GOLDONE. E perché, di grazia, un soggetto a rischio, come ad esempio un maschio gay, si vaccina per
@LazzaroDelPrete - Lazar Kaganovich
5. Il monkey pox? Per scopare SENZA GOLDONE, mi pare chiaro. Bene, sarà esposto a candida, condilomi/papilloma, epatite C, HIV, sifilide e tanta bella robina che non vale la pena elencare. Vaccino morbillo e monkey pox funzionano? Si, benissimo. Ha senso farli? No. Allo
@LazzaroDelPrete - Lazar Kaganovich
6. Stesso modo, la chemioterapia ha rivoluzionato le strutture, perché certi farmaci antiblastici (quasi tutti) sono orribilmente tossici. Quindi, ci si è trovati a dover creare percorsi, UFA (reparti di farmacia isolati e trattati a parte), formazione, dpi, info ai
@LazzaroDelPrete - Lazar Kaganovich
7. Parenti, perché diventano tossici anche pupu, pipí e sudore. Campagne di campionamento e tamponi sulle superfici dei reparti. Di cui, tra le altre cose, mi occupo. Reparti semi isolati, e così via. Chi se ne occupa, a livello dirigenziale? Medici specializzati in igiene
@LazzaroDelPrete - Lazar Kaganovich
8. E medicina preventiva. Specialistica che NESSUNO vuole fare. Cosa se ne deduce? Che ci vuole la VOLONTÀ di fare le cose. De Donno, di cui ho ancora il cellulare, e che dovevo intervistare, si è ucciso perché trattato da ciarlatano, sulla base del fatto che soggetti
@LazzaroDelPrete - Lazar Kaganovich
9. Col cervello lavato in campo scientifico, politici di 4to livello e analfabeti funzionali col blog, o pagati (in 3 o 4 passaggi, ne parleranno in tribunale) dalle case farmaceutiche hanno creato un clima per cui era de facto VIETATO curare. Censurando sui social, ma
@LazzaroDelPrete - Lazar Kaganovich
10. Sempre senza saperne un cazzo, come puénte (che sarebbe ininfluente), o peggio sospendendo e radiando professionisti per partito preso, senza dati perché troppo presto, gestendo tutto in deroga non solo della democrazia, ma della scienza stessa. Che si basa sul
@LazzaroDelPrete - Lazar Kaganovich
11. NON CREDERE a niente di non sperimentabile o riproducibile. Avete voluto fare una religione, basata sulle menzogne di chi fa dividendi sulla salute delle persone. Poco importa se il vaccino Covid funzioni o no, personalmente ritengo di sì, ma poco (e tanto non si può sapere:
@LazzaroDelPrete - Lazar Kaganovich
12. Nessuno si è mai sognato di rilevare i dati dei pazienti vaccinati ammalati sul piano della storia clinica, chessò, peso, diabete, cardiopatie pregresse eccetera), ed essendo un intervento PREVENTIVO sul piano statistico si possono solo fare ipotesi, non esistendo
@LazzaroDelPrete - Lazar Kaganovich
13. Fisiologicamente controfattuali possibili. Poco importa anche degli eventi avversi, ma solo se una rilevante efficacia è dimostrata... Quotidianamente si ragiona in termini di costi/benefici. Il peccato originale del vaccino in pandemia è stato il totale e insensato
@LazzaroDelPrete - Lazar Kaganovich
14. Distacco dall'epistemologia. Per dare, anzi lasciare il monopolio della voce al dogma. Che, va detto, finché lo scrive un medico come Bassetti o Burioni, posso anche tenerlo in considerazione. Ma sempre tenendo stretti Cartesio e Galileo. Se però il dibattito prevede
@LazzaroDelPrete - Lazar Kaganovich
15. Interventi di Selvaggia Lucarelli, Brindisi, Bizzarri, e devo vedere puénte che rompe il cazzo a un luminare con 35 anni di clinica come Stramezzi, dall'alto di stocazzo in quanto vergine di nozioni di medicina, non ci sto più. Bene che le iene si sveglino, ma lo
@LazzaroDelPrete - Lazar Kaganovich
16. Fanno perché fiutano l'aria, e sono la stessa demagogia di merda di un Report che fa le liste di proscrizione col coglione Orlowski. Ma si deve ripartire. E la fiducia verso la classe medica non si è certo persa per colpa dei novax (altra categoria semantica buona
@LazzaroDelPrete - Lazar Kaganovich
17. Per i bambini scemi, che va dallo psicotico terrapiattista al professionista possibilista ma scettico come me, che non sono certo contrario per partito preso, lavorandoci e avendoci lavorato, e tu Merdoso rileggiti il mio Cv). Bensì dagli avvelenatori di pozzi.
@LazzaroDelPrete - Lazar Kaganovich
18. State tranquilli. In sanità, il dibattito non va in televisione. Recuperate la fiducia in chi vi cura, denunciate chi non lo fa, ma non certo quelli che non vi curano come dite voi. I medici GIURANO FEDELTÀ A UN PRINCIPIO. E al servizio che fanno. Crollano, muoiono sul
@LazzaroDelPrete - Lazar Kaganovich
19. Lavoro, si suicidano, a volte devono scappare per la fatica. Il 99,9%. Ripartiamo dal senso di comunità e di civiltà, ed isoliamo mestatori, truffatori e propagandisti prezzolati e ignoranti. Non è certo la #FabbricaOdio a decidere per voi.
@LazzaroDelPrete - Lazar Kaganovich
@threadreaderapp please unroll
@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
1. 💥 L'email di Noël Wathion vicedirettore di EMA il 19 novembre 2020, prova le pressioni di Ursula von der Leyen per l'approvazione immediata dei VACClNl. Il giorno dopo firmò il contratto UE da 300 milioni di dosi in cui Pfizer che le conseguenze erano sconosciute. Thread

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
2. Noël Wathion parla di un’atmosfera non solo “abbastanza tesa” ma “a volte anche un po’ scomoda”. Un ritardo di diverse settimane tra l’approvazione USA e quella UE “forse non è facile da accettare” per la Commissione UE perché “le conseguenze politiche” sarebbero elevate.

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
3. Wathion descrive questa enorme pressione temporale come un conflitto tra il processo di approvazione “accelerato” richiesto politicamente e l’obbligo della sua autorità di prendersi il “tempo necessario” per avere “solida certezza” sulla sicurezza del VACClNO.

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
4. EMA approvò i VACClNl nei tempi politici invece che in tempi scientifici. Anche l'email di Alexis Nolte, capo di Human Medicines di EMA, sollevano perplessità sul metodo di approvazione e sulla rapidità con cui EMA si è liberata dei dubbi che aveva fino a pochi giorni prima.

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
5. L'email di Evdokia Korakianiti, amministratore scientifico dell’EMA, spiega in modo più dettagliato quali fossero questi “problemi” e come fossero in realtà le principali preoccupazioni legate al VACClNO Pfizer-BioNTech. https://www.nius.de/corona/diese-dokumente-zeigen-den-impf-pfusch-bei-der-zulassung-qualitaet-derzeit-als-nicht-akzeptabel-befunden/72538f37-bf65-45f4-b4c2-b4394bf35d0a



@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
6. Marco Cavaleri, responsabile dei VACClNl di EMA, comunicava con urgenza come FDA statunitense "si precipiterà nell'Autorizzazione di Emergenza (EUA)". https://archive.is/sQYoE

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
7. Wathion, scrive in modo scioccante, come "le ricadute politiche per un ritardo sembrano essere troppo elevate" e se i tempi non saranno rapidi come quelli di FDA "saremo travolti su tutti i fronti e ci troveremo nel mezzo della tempesta."

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
8. Ciò implica che la velocità a scapito della sicurezza era all'ordine del giorno per evitare "ricadute politiche". Chiaramente, è stata la politica a dettare il protocollo di autorizzazione, non la scienza.
@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
9. Marco Cavaleri di EMA rivela che Albert Bourla CEO di Pfizer ha "fatto pressioni" su Peter Marks direttore del Center for Biologics Evaluation (CBER) di FDA. L'accesso della Pfizer a FDA solleva dubbi sull'indipendenza dell'agenzia federale.

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
10. Cavaleri rivela che FDA era a conoscenza di "alcuni problemi" associati alla CMC (Chimica, Produzione e Controll) che dovevano essere risolti e che potrebbe "essere la parte difficile". LA CMC copre procedure garantire la sicurezza e la coerenza tra i lotti farmaceutici.

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
12. Veronika Jekerle, responsabile della qualità della farmaceutica di EMA, scrive a Evdokia che la differenza nel livello di integrità dell'mRNA è stata nuovamente segnalata come una delle principali preoccupazioni e il suo "potenziale impatto sulla sicurezza".

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
13. Marco Cavaleri scrive che il contenuto di mRNA non è la maggiore preoccupazione di FDA e afferma inoltre in modo scioccante: "non è chiaro se le ispezioni di GCP (Buona Pratica Clinica) siano mai state effettuate" e non sembra il maggiore interesse di FDA.

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
14. Jekerle Veronika rivela che EMA, FDA, MRHA e Health Canada (HC) sono tutte infromate della bassa integrità del mRNA, ma nessuno sembra preoccupato per la sicurezza. https://www.nius.de/Corona/jetzt-ermittelt-sogar-der-us-bundesstaat-texas-die-chronik-der-pfizer-skandale/2029fe4b-e598-46d8-b82d-0cbce2b8f979

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
15. In un rapporto trapelato del'incontro di Pfizer e EMA il 26 novembre 2020, un giorno dopo l'email di Jekerle, rivela come hanno risulto il problema dell'integrità dell'mRNA: Abbassando il limite al 50%, inferiore alla soglia minima del 70% prevista da Acuitas Therapeutics. https://t.co/ru7WHyZrWT

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
16. "L'mRNA troncato dovrebbero essere considerato impurità legate al prodotto. Dovrebbe essere affrontata la possibilità che proteine tradotte diverse dalla proteina sSpike prevista (S1 S2) risultino da specie di mRNA troncate e/o modificate". https://t.co/M1SdBlj4nG

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
17. Occorre ricordare che il trial Pfizer fu effettuato con lotti clinici speciali di alta qualità con un'integrità del 78%, prodotti con un processo diverso da quello industriale usato per i lotti commerciali. Nel trial solo 252 su 21.720 ricevettero il lotto commerciale. https://t.co/5kBy34cca4

@ChanceGardiner - Chance 🤺 Giardiniere 🍊 🔞
18. Noël Wathion vicedirettore esecutivo di EMA fu mandato in pensione il 30 giugno 2021 dopo 25 anni di servizio ed è deceduto il 12 agosto 2023. Così nessuno può più chiedergli nulla sulle pressioni su EMA da parte di Ursula von der Leyen e probabilmente da parte di Pfizer. https://t.co/eJ0MLByaTG


@Adriano72197026 - Adriano Valente
Ecatombe Vaccinale avanza 🧪⚠️ PFIZER DA GUINNESS Di REAZIONI AVVERSE ✔️ 575 PAGINE per dire che non sanno nulla. Download 📥 bugiardino 🤥: aifa.gov.it/comirnaty https://t.co/Pu6CRsVKQ0


@biologyphen0m - D
Scottish COVID inquiry|Day 21 part-4 'they found my father on his hands and knees trying to get to the toilet' 'I was then told they were going to introduce end of life medication which would be MIDAZOLAM and if needed MOPRHINE' 'i was SHOCKED !' Cause of death COVID-19 https://t.co/qUDdVO1tMi

@robinmonotti - Robin Monotti
NURSE WHISTLEBLOWER LESLEY ROBERTS ON 2020 "COVID DEATHS" IN NHS SCOTTISH HOSPITALS: "If they had breathing difficulties then their breathing was being suppressed even further by the drugs and it was this that then killed them, not Covid." The death protocol: Covid whistleblower Lesley Roberts believes this one medical blunder cost thousands of lives "It relates to the NG163 'end of life' protocol from NICE, the National Institute for Health and Care Excellence. It was issued to doctors and nurses across the UK on April 3, 2020 and remained in place until March 21, 2021 According to Ms Roberts and other healthcare campaigners, NG163 essentially told medics to prescribe a deadly cocktail of powerful drugs to people in hospital and elsewhere who had been diagnosed with an advanced case of Covid-19. She said: "It should never have been considered. People who were not at the end of their lives were brought to the end because of those drugs. If they had breathing difficulties then their breathing was being suppressed even further by the drugs and it was this that then killed them, not Covid." #Midazolam


@nesta_red - Nesta Red
#Deaths:2020..#Depopulation vs the #Holocaust. The #Covid #Killing #Protocols(2020)+"#Vaccine"(21+22) #bioweapons≃1.7 times the Holocaust. 31mil vs 18mil. By country: https://tumia.org/en/directory/en/instance.php?tiname=Covid%20World%202022-10-09:%203%20Years%20of%20Cov-Vaccine%20Bioweapons:%20Estimated%20Extra%20Deaths%2031M-Adv.%20Eff.%201.9B&relationship=All&drsid=0&pisid=0&tiname_dno=1&page=1 https://en.wikipedia.org/wiki/Holocaust_victims #Nuremberg2 #vaccineholocaust

@nesta_red - Nesta Red
#Deaths of the 2020..#Depopulation vs the #Holocaust.The #Covid(2020)+"#Vaccine"(21+22) #bioweapons≃1.7 times the Holocaust. 31mil vs 18mil. By country: https://tumia.org/en/directory/en/instance.php?tiname=Covid%20World%202022-10-09:%203%20Years%20of%20Cov-Vaccine%20Bioweapons:%20Estimated%20Extra%20Deaths%2031M-Adv.%20Eff.%201.9B&relationship=All&drsid=0&pisid=0&tiname_dno=1&page=1 https://en.wikipedia.org/wiki/Holocaust_victims #Nuremberg2 #nazis #vaccinegenocide #vaccineholocaust
@robinmonotti - Robin Monotti
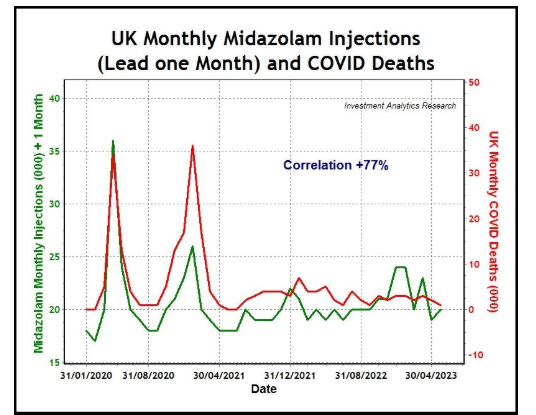
'Excess Deaths in the United Kingdom: Midazolam and Euthanasia in the COVID-19 Pandemic': "This paper shows that the UK spike in deaths, wrongly attributed to COVID-19 in April 2020, was not due to SARS-CoV-2 virus, which was largely absent, but was due to the widespread use of Midazolam injections which were statistically very highly correlated with excess deaths in all regions of England during 2020. The widespread and persistent use of Midazolam in UK suggests a possible policy of systemic euthanasia... UK excess deaths were closely associated with the use of Midazolam and other medical intervention. The iatrogenic pandemic in the UK was caused by euthanasia deaths from Midazolam and also, likely caused by COVID injections..."


@TheRustler83 - Rustler
Monthly Midazolam doses V Monthly Deaths (Age 75+) England 2019-2021 🚨 32,000 #ExcessDeaths in April 2020 +112% above 5-year average 🚨 Midazolam doses up +131% in April 2020 Our elderly weren’t dying from COVID- they were systemically assaulted with End-Of-Life protocols 1/

@TheRustler83 - Rustler
Monthly Midazolam doses V Excess Deaths (Age 75+) England 2019-2021 🚨 55,000 #ExcessDeaths in 2020 +20% above 5-year average (Age 75+) 🚨 60,000 Excess doses of Midazolam given in 2020 These were not ‘COVID’ deaths NICE NG163 End-of-life protocol 2/

@TheRustler83 - Rustler
Monthly Modazolam doses V Age-standardised mortality rates (Age 75+) 🏴England 2019-2021 There is no hiding place here - age standardised rates are the gold standard - and they DOUBLED in April 2020 We also see a second correlation spike over Christmas/New Year 2020/21 3/

@TheRustler83 - Rustler
Excess Midazolam % Vs Excess Death % (Age 75+) England 2020-2021 April 2020 🟧 Midazolam +131.5% 🟦 Excess Deaths +112.8% January 2021 🟧 Midazolam +57.5% 🟦 Excess Deaths +27.7% How to create the illusion of a pandemic …. 4/

@TheRustler83 - Rustler
Source no.1 NHS OpenPrescribing #Midazolam usage, past 5 years 5/ https://openprescribing.net/chemical/1501041T0/

@TheRustler83 - Rustler
Source no.2 ONS Monthly mortality analysis 6/ https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/monthlymortalityanalysisenglandandwales

@TheRustler83 - Rustler
Credit to Dr Wilson Sy for posting his paper: ‘Excess Deaths in the United Kingdom: Midazolam and Euthanasia in the COVID-19 Pandemic’ I wanted to focus on the most vulnerable age group- the elderly- to take a deeper look at the correlation with excess 7 https://www.researchgate.net/publication/377266988_Excess_Deaths_in_the_United_Kingdom_Midazolam_and_Euthanasia_in_the_COVID-19_Pandemic


@TheRustler83 - Rustler
“The UK COVID-19 pandemic was iatrogenic, created with widespread and persistent use of Midazolam injections in all regions of England, particularly in care homes, under a systemic policy of euthanasia” 🟩 Monthly Midazolam use 🟥 COVID Deaths 8/ https://t.co/RD3gI7cQNK

@TheRustler83 - Rustler
The anomaly of excess deaths in April 2020 is clear evidence of Lockdown harms ‘COVID’ cases were low at this time yet this was our highest month of death during the pandemic These were deaths caused by the COVID-treatment & response protocols Why else did deaths just stop? 9 https://t.co/1eDOemv2TY

@TheRustler83 - Rustler
17 April 2020 Health Secretary Matt Hancock & Dr Luke Evans MP, openly discuss what is needed for: A Good Death Telling us in plain sight You are still on the list, Matty 10/ #Midazolam
@TheRustler83 - Rustler
🏴 Scotland 2020/2021 🟪 Excess deaths in care homes 📊 Midazolam usage 3,000 excess deaths during lockdown - blamed on ‘COVID’ After lockdown ‘COVID’ disappeared for the summer - returning after the FLU vaccine roll out in September 2020 https://t.co/OU1yK3Xi4U


@TheRustler83 - Rustler
@TheRustler83 - Rustler
For those 32,000 excess deaths in April to have been ‘COVID’ deaths the IFR needed to be 25% The actual IFR of deaths attributed to COVID is now known to be 0.1% Something else was killing those old folks Was it the COVID-protocols rather than ‘COVID’ Read NG163 https://t.co/Vt22UlwT6l


@MISSXBUTTERFLYX - missbutterfly 🌸
The truth is coming of Nhs murder/manslaughter ‼️‼️ #Midazolam Were Covid patients left to die against their wishes? Care homes under pressure to issue Do Not Res… https://mol.im/a/13277723 via https://dailym.ai/android


@ABridgen - Andrew Bridgen MP
“He FaceTimed me. He looked really well. He was up and dressed… he was laughing and joking.” Widow Lianne Menzies tells the Scottish Covid Inquiry how her 38 year old husband Jamie was getting better, was given Midazolam “to help him sleep”, then died. Experienced nurse John Campbell: “I’ve never, ever in forty five years of nursing given Midazolam to help someone sleep.” What on earth went on in care settings with Midazolam during the pandemic? The English Covid Inquiry, meanwhile, is fearlessly grilling Sue Gray about Westminster gossip. Shameful. https://www.youtube.com/watch?v=eHBpD7cuNB4&t=131s


@CartlandDavid - Dr David Cartland BMedSci MBChB MRCGP (2014)
UK pandemic deaths caused by euthanasia drug Midazolam, new research paper claims | Total Health https://www.totalhealth.co.uk/blog/uk-pandemic-deaths-caused-euthanasia-drug-midazolam-new-research-paper-claims
@TheRustler83 - Rustler
🚨🚨 9 times out of 10 Care Home residents were prescribed ‘End of Life’ medication during Lockdown What followed was 5,000 deaths in just 10 weeks at Scottish Care Homes and 50,000 in England…..
@TheRustler83 - Rustler
Just-In-Case medication = Anticipatory Care medicine= End-of-Life drugs It’s just a nicer way of saying “We are going to kill you now”

@TheRustler83 - Rustler
Link to the full transcript + witness statements from the day⬇️ https://www.covid19inquiry.scot/hearing/impact-hearing-health-social-care-day-30

@TheRustler83 - Rustler
From the same day at the Inquiry 26/3/2024 This should have brought the entire house of cards crashing down 0 (zero) media coverage of those testimonies
@TheRustler83 - Rustler
Midazolam Matt Hancock April 2020
@TheRustler83 - Rustler
Scottish Covid Inquiry | Full Documentary | https://youtu.be/bojR7A5MKPA?si=faXtUa_OCIRumdFk
@TheRustler83 - Rustler
Care Home Excess Deaths in 2020 🏴🏴 No excess before lockdown 100% excess during lockdown No excess after lockdown https://t.co/VVNTUWYZ0h


@TheRustler83 - Rustler
DO NOT RESUSCITATE
@TheRustler83 - Rustler
People asking where the directive came from: Straight from the NHS/NICE
@TheRustler83 - Rustler
“Sedation and opioid use should NOT be withheld because of an inappropriate fear of causing RESPIRATORY DEPRESSION” COVID-19 rapid guideline: managing symptoms (including at the end of life) in the community NICE guideline NG163 Published: 3 April 2020 https://files.elfsightcdn.com/5266f37f-1e60-4e3b-9202-0f9e41473266/2a4df24d-b4c4-4056-aec6-c4bbd5c11090.pdf https://t.co/pRel3HLhaq


@TheRustler83 - Rustler
#Midazolam
@TheRustler83 - Rustler
Human Rights Act
@TheRustler83 - Rustler
COVID MISATTRIBUTION

@chrislittlewoo8 - Chris Littlewood
🧵: THEY KNEW. THEY LIED. THEY MURDERED THEM. 1/ Every time I go back to this, it makes me sick. The elderly in care homes were not cared for. They were systematically killed with Midazolam and Morphine and their deaths were falsely recorded as COVID to fuel a manufactured crisis.
@chrislittlewoo8 - Chris Littlewood
2/ Since 2021, many of us have been exposing this. We were ridiculed, ignored, and silenced. But now, with a senior coroner confirming the truth, the cover-up is crumbling. The state executed the vulnerable and called it a pandemic.
@chrislittlewoo8 - Chris Littlewood
3/ HOW THEY DID IT: The government issued guidelines pushing the use of Midazolam and Morphine in care homes. These drugs were given via syringe drivers, ensuring a continuous, unrecoverable dose.
@chrislittlewoo8 - Chris Littlewood
4/ If you have breathing difficulties, Midazolam and Morphine do not ease your suffering. They suffocate you. The combination depresses your central nervous system until your lungs fail completely.
@chrislittlewoo8 - Chris Littlewood
5/ This was not some gentle drifting off into the night. This was not peaceful palliative care. It was the medical equivalent of waterboarding someone to death.
@chrislittlewoo8 - Chris Littlewood
6/ Imagine drowning, but instead of water filling your lungs, it's your own body's failure to inhale. You try to breathe, but your muscles do not respond. Your lungs are paralysed. Your brain screams for oxygen. But nothing happens.
@chrislittlewoo8 - Chris Littlewood
7/ That is how they died. Slowly. Silently. Terrified. And then their deaths were signed off as COVID to justify lockdowns, emergency powers, and a global vaccination campaign.
@chrislittlewoo8 - Chris Littlewood
8/ Many of these people were not terminally ill. They were not dying from COVID. But they were written off, given fatal doses, and left to die in silence—alone, isolated from their families.
@chrislittlewoo8 - Chris Littlewood
9/ What was happening in hospitals at the same time? Ventilators, Remdesivir, and DNRs, protocols designed to kill. At every stage, the goal was death.
@chrislittlewoo8 - Chris Littlewood
10/ They NEEDED the death numbers to justify what they were doing. Lockdowns, mass testing, mail-in ballots, vaccine rollouts, all of it relied on creating a perception of mass death.
@chrislittlewoo8 - Chris Littlewood
11/ If people had recovered, the fear campaign would have failed. If people had lived, they couldn’t have called it a pandemic. Instead, they euthanised them and sold it as a humanitarian crisis.
@chrislittlewoo8 - Chris Littlewood
12/ The legal case is now undeniable. The guidelines were there. The prescriptions were there. The syringe drivers were there. The false death certificates were there.
@chrislittlewoo8 - Chris Littlewood
13/ This was not incompetence. This was premeditated mass murder. A government-orchestrated culling of the elderly, hidden in plain sight.
@chrislittlewoo8 - Chris Littlewood
14/ And now, the coroner’s confirmation is exposing it all. The same system that tried to cover it up is now being forced to admit what was done.
@chrislittlewoo8 - Chris Littlewood
15/ But we knew years ago. We were screaming about this in 2021. We saw it, we called it out, and we were ignored. Now the world is catching
@chrislittlewoo8 - Chris Littlewood
16/ So what happens next? Do we let them walk away from this? Do we allow them to rewrite history? Or do we demand justice for the thousands of lives they stole?
@chrislittlewoo8 - Chris Littlewood
17/ This is bigger than COVID. This is about a system that executed its own citizens and then lied to the world about it.
@chrislittlewoo8 - Chris Littlewood
18/ If we do not stand for those murdered in care homes, then who will? If we do not expose this, it will happen again.
@chrislittlewoo8 - Chris Littlewood
19/ Justice is coming. And when it does, those responsible must face consequences so severe that nothing like this can ever happen again.
@chrislittlewoo8 - Chris Littlewood
20/ Share this thread. Make noise. Do not let them bury this.
@chrislittlewoo8 - Chris Littlewood
EVIDENCE (numbered to match the thread, fully comprehensive) 1️⃣ Government protocol to remove elderly & disabled from hospitals back into the community 📄 Source: https://tinyurl.com/5dcfap57
@chrislittlewoo8 - Chris Littlewood
2️⃣ Protocol stopping elderly & disabled from gaining hospital care 📄 Source: https://tinyurl.com/ycku67wm
@chrislittlewoo8 - Chris Littlewood
3️⃣ COVID Decision Support Tool (Scoring Matrix) – Who gets treatment, who gets left to die 📄 Source: https://tinyurl.com/4hsxhyn9
@chrislittlewoo8 - Chris Littlewood
4️⃣ Investigation into mass DNR orders that placed people on End-of-Life care pathways 📄 Source: https://tinyurl.com/39r4re5m
@chrislittlewoo8 - Chris Littlewood
5️⃣ NICE Protocol NG163—a step-by-step manual for dealing with COVID+ people in the community 📄 Source: https://tinyurl.com/795tpym9
@chrislittlewoo8 - Chris Littlewood
6️⃣ NHS End-of-Life protocol—same Midazolam dosage for "anxiety" as for euthanasia 📄 Source: https://tinyurl.com/2p8kk8kk
@chrislittlewoo8 - Chris Littlewood
7️⃣ BNF (British National Formulary) Midazolam dosage guide and known respiratory suppression risks 📄 Source: https://bnf.nice.org.uk/drugs/midazolam
@chrislittlewoo8 - Chris Littlewood
8️⃣ UK Government purchased 2 years' supply of Midazolam in weeks – proving premeditation 📄 Source: https://questions-statements.parliament.uk/written-questions/detail/2023-11-22/3234
@chrislittlewoo8 - Chris Littlewood
9️⃣ Maajid Nawaz: Senior coroner confirms Midazolam played a role in deaths 📄 Source: https://open.substack.com/pub/maajidnawaz/p/breaking-senior-coroner-confirms
@chrislittlewoo8 - Chris Littlewood
🔟 "A Good Death"—A documentary on how people were murdered with Midazolam 📄 Source: https://ugetube.com/watch/a-good-death-jacqui-deevoy-ickonic_mbVzww3HAB6o35v.html
@chrislittlewoo8 - Chris Littlewood
1️⃣1️⃣ UK Government discussing the use of Midazolam to ensure "A Good Death" 📄 Source: https://t.co/4M49PemEnv
@chrislittlewoo8 - Chris Littlewood
@threadreaderapp unroll please