reSee.it - Related Post Feed

@VictorFromDE - Victor Scott
This thread covers the deadly hospital protocols. Not just Remdesivir but other sedatives, drugs, DNRs, lack of food & water, etc. Many saying they have lung injuries or "long Covid" can thank these protocols. This is a video of Nicole Sirotek, one of the 1st to expose this. /1 https://t.co/nHeXF4GR04
@VictorFromDE - Victor Scott
A nurse named Erin went undercover and recorded what was happening. This was also very early on in the plandemic. /3 https://t.co/kQdT261Mq7
@VictorFromDE - Victor Scott
More testimony from nurses, family members, etc. on the deadly protocols. /5 https://t.co/LXZV8wJyMO
@VictorFromDE - Victor Scott
Yet another nurse describing what she witnessed. https://t.co/6Q7HQeGUTz

@brixwe - .。.☆ 𝔼𝕞𝕞𝕪 ☆.。.
Nurse speaks out about how they deliberately KILLED patients during the Covid Dark Age putting healthy patients on ventilators to add numbers.

@annabeth9691 - annabeth
Very brave nurse and veteran standing up! Hospital protocol kills!!! #COVID19 #CrimesAgainsHumanity #accountability (make sure to watch all 4 parts)

@SaiKate108 - Kat A 🌸
Courageous San Francisco nurse Gail McCrae has tales to tell about the shocking 3 fold increase in hospitalisations/deaths she witnessed directly associated with the vaccine rollout. Most astonishing was the dramatic increase in code blues from 1 code blue per shift to 6-10. Most coming from the vaccine clinic. Staff were warned not to report on adverse events and unfortunately most complied. Gail was fired from her job and taken out of her graduation program for speaking out. Her story deserves to be heard!! https://rumble.com/v36uula-medicine-failed-us-nurse-gail-mccrae.html

@DocAhmadMalik - Dr Ahmad Malik
Listen to this senior hospital manager describe what it was like in a major teaching hospital in central London at the height of the Plandemic. Do not fall for the lies.

@CBKNEWS121 - CBKNEWS
BOMBSHELL: Nurse testifies that none of the millions of covid patients died from covid, they died from medical mal-practice... hospitals were made to follow government orders that led to the deaths of millions of people... confirmed genocide... nuremberg 2.0 trials needed... #Covid

@RealPatrickWebb - Patrick Webb
BOMBSHELL: Hospitals were forced to execute government directives that resulted in the deaths of millions of people, confirming genocide and calling for Nuremberg 2.0 trials, according to a nurse who testified that none of the millions of patients with COVID died from COVID; they died from medical malpractice.

@wolsned - DD Denslow 🇬🇧
"I didn't see a single patient die of covid' Frontline Nurse Nicole Sirotek State sponsored murdered, from cradle to grave.

@catsscareme2021 - Jessica Rojas 🇺🇸💪
Written by a NICU nurse. "I am a neonatal intensive care unit (NICU) nurse. For almost 14 years I worked in some of the best children’s hospitals in the country. I have never really been one to question “modern medicine” until somewhat recently. When you work in healthcare, you mostly just assume that everything is research-based, done with purpose, and done for the ultimate good of the patient. “First, do no harm”, right? I think having my own child and realizing the gravity of my decisions regarding his care have made me dig very VERY deep into the research behind what has come to be second nature to the majority of us: vaccines." "I am not a crazy, emotionally-driven person. I think anyone reading this knows me well enough to appreciate that about me. My husband will tell you that I research things to death – it’s true. I don’t watch TV and I couldn’t care less about what Hollywood celebrities have to say about any topic. I never was even interested in the autism aspect/argument, and that is not at all what led me to start looking into vaccine research. It was actually one of my best friends who is a critical care pediatric nurse practitioner – she was always in favor of vaccines, worked in cardiac ICU and oncology units in reputable children’s hospitals and thought it was crazy not to vaccinate your kids. Flash forward to today and none of her children are vaccinated. She is one of the smartest, most well-read and well-researched people I know. She has written medical journal articles and has contributed chapters to medical textbooks. She does NOT make decisions without a great deal of research, thought and prayer. So when she did a 180 on vaccines, I listened. And I began to research on my own." I went from spending 14 years of my nursing career giving vaccines to my patients and thinking parents who didn’t vaccinate were irresponsible and crazy, to now recognizing the great harm that is being done to our children by the vaccine industry. Autoimmune disease, asthma, eczema, food allergies (especially peanut), seizure disorders, learning disabilities, chronic ear infections, allergies – all these health issues are running rampant in our kids. I witnessed countless occasions of vaccine injury in the NICU, and the truly disturbing part is that it is considered “normal”. We would vaccinate babies and then inevitably that night or the next day the baby would have increased apnea spells (they would stop breathing), they would require increased ventilator support, they’d have more feeding difficulties or higher amounts of gastric residual/vomiting. The doctors were never surprised. This was just an expected response to vaccination. This was the standard in every NICU I worked in (that would be 6 different NICUs all over the country). I also never ONCE, not in 14 years, observed a doctor giving true informed consent to parents regarding vaccinating their baby. It was our job as the nurse to get the parents to just sign the consent form after handing them a printed off sheet from the CDC which was strongly biased toward vaccination. If you were told the truth that your baby could stop breathing after getting vaccines, would you perhaps question it? Or at least ask to postpone until they are older? If you as a parent aren’t 100% certain that the medical intervention you are giving your child is safe and healthy for them, then you have the right (and the responsibility) to say no. Ask to wait. Ask to delay until you research further. You can always vaccinate later. You can never UN-vaccinate. Every state allows for vaccine exemptions for your child to attend public school. Most allow for religious or conscience exemptions (47 states) in addition to medical exemptions. I am not demanding that you stop vaccinating your kids. I am simply urging you to question. Do your own research. Find sources that aren’t bought and paid for by the pharmaceutical industry. Make sure there aren’t conflicts of interest. "
@catsscareme2021 - Jessica Rojas 🇺🇸💪


@stkirsch - Steve Kirsch
A NICU Nurse Turns Vaccine Whistleblower. This is from 2018. It’s a short read. Please read and repost. You’ll save lives. https://paleofam.com/2018/08/a-nicu-nurse-turns-vaccine-whistleblower/
@stkirsch - Steve Kirsch
From a nurse friend of mine: I can attest to this NICU nurse. I NEVER consented parents when I gave them the Hep B vaccine or Vit K on the first day of life. On the contrary if they refused I would have to make them sign a consent that they were going against the recommendations. But as labor and delivery nurses we questioned why it was necessary a one day old baby needed the hep b vaccines. No pediatrician could give us a good answer. So my best way of consenting parents without getting in trouble was to have the parents ask all the labor and delivery nurses if we gave our children the hep B vaccine when making their choice. And the answer was always NO. We knew it wasn't right because it didn't make sense if parents were Hep B negative. I would ask the question if they were concerned about their newborn babies going out and having unprotected sex and the answer was no. It never made sense to us nurses. We were just being forced to do what was protocol.

@MakisMD - William Makis MD
NEW ARTICLE: NURSES collapsing with Cardiac arrests, blood clots, aneurysms, dying in sleep, Turbo Cancers and Sudden Deaths - 100 Nurses Injured & dead (since May 2023) This is the Largest compilation of Nurses injured & killed by COVID-19 Vaccines ever published! 100 NURSES. Since May 2023! Dec.5, 2023 - Concord, NH - 23 year old Andy Hoang was in 1st year of her nursing job - she suffered a cardiac arrest during training session on how to respond to someone in cardiac arrest (I honestly didn’t make this up) Dec.5, 2023 - Colorado cardiac nurse Jennifer Harlan survived her 3rd heart attack. She works in cardiac unit. Dec.2, 2023 - Cherrybrook, NSW, Australia - 36 year old neonatal ICU nurse Amy Barker and her unborn boy Marcus both died suddenly and unexpectedly with baby at 36 weeks. Family has no answers. Dec.2, 2023 - Seattle, WA - Sonya Denise Holden has suffered a brain aneurysm. “I had COVID 4 times and three COVID shots.” (I'm also not making this one up either) Nov.14, 2023 - Castle Rock, CO - Karen Andrews, a nurse, was just diagnosed with very aggressive breast cancer that is growing so quickly, doctors had to abandon surgery and go straight to chemo Nov.5, 2023 - TX - 53 year old Kathleen Ann Martinez, “Winner of Best Nurse of South Texas”, died suddenly after 7 month battle with cancer. Nov.2, 2023 - NY - 34 year old Kristina Ferraro, Pediatric Nurse and former EMT, died after a battle with Colon Cancer. Nov.1, 2023 - New Haven, CT - Nurse Jackie Jermine was diagnosed with Acute Myeloid Leukemia on Nov.1, 2023. Lot 011J20A Moderna COVID-19 mRNA Vaccine. Oct.23, 2023 - US ARMY NURSE DEAD - Liberty Hill, TX - 42 year old Krista Labbe, Lieutenant Colonel US Army Nurse Corps died suddenly on Oct.23, 2023. Oct.19, 2023 - New Lenox, IL - Sheila Bennett-Holloway is an LPN (licensed practical nurse) She is now suffering from a 2nd cancer in the past year, recurrent infections, bowel obstruction, etc. 100 in TOTAL in this groundbreaking work. ASSESSMENT: Nurses and Teachers are the two professions that are getting completely annihilated by COVID-19 mRNA Vaccine mandates and the lethal effects those mandates continue to have to this day. Why do I do these compilations? It’s a record of the devastation that these toxic COVID-19 mRNA Vaccines have brought upon our world. In an era of fake obituaries, woke Artificial Intelligence programmed by Communists, 3-letter intelligence or government agencies, and out of control censorship, individual deaths can be scrubbed from the internet, disappeared, and completely forgotten. You can actually test this yourself. Type “Nurse died 2023” into Google Images. I guarantee you that 99% of the nurses in this compilation will not show up in the GOOGLE search. That is the level of censorship we are in right now. 99% is hidden, removed, scrubbed. If you just do a quick search, 99% of these people don't even exist - Google will hide them so you never see them! In this compilation there are: 47 cancers (many at Stage 4) 12 cardiac arrests 8 died in sleep 5 blood clots 5 are veterans who served in the military 3 were pregnant & injured or died 2 had aneurysms 1 collapsed & died behind the wheel of a car There is probably a bias towards noticing cancers or deaths due to cancer, so that group of injuries is likely over represented. This is not a scientific assessment, as we are dealing with incomplete information. Nevertheless, that’s almost 50% of nurse injuries & deaths due to cancer alone, which is absolutely horrifying. Most of these cancers are TURBO CANCERS - and we urgently need COVID-19 Vaccinated people to wake up to the dangers of Turbo Cancer, start taking cancer prophylaxis and protection and we need pathologists to start staining tumors for mRNA and spike protein. Stop being worried about your jobs and your boat payments, it's time to start being doctors again. Article Link in photo to avoid shadowban, just re-type the URL into your browser to access Special thanks to: @tulloch1978 @resilient333 @toobaffled @JonelessHomes @vancemurphy @VigilantFox @TheChiefNerd @NaomirWolf @twc_health #DiedSuddenly #cdnpoli #ableg


@ClaudiaMonet67 - Claudia Monet 👻🦩🛵🌿🧉☕️🚀
Never forget that they did not let you see your loved ones when they were dying never forget, they did not allow anyone in the hospital room when women were having their babies all alone NEVER FORGET!!
@denisrancourt - Denis Rancourt
Nurse Gail Macrae is the most credible high-quality witness of hospital-industry organized criminality I have even heard This 20-minute interview is vital information and analysis to understand the magnitude of the structured assault against the domestic population A MUST-WATCH FOR ALL RESEARCHERS Source with article: https://childrenshealthdefense.org/defender/gail-macrae-california-icu-nurse-covid-protocols-vaccine-injuries/ Source for video: https://rumble.com/v4120pk-covid-nurse-speaks-out.html #gailmacrae



@CartlandDavid - Dr David Cartland
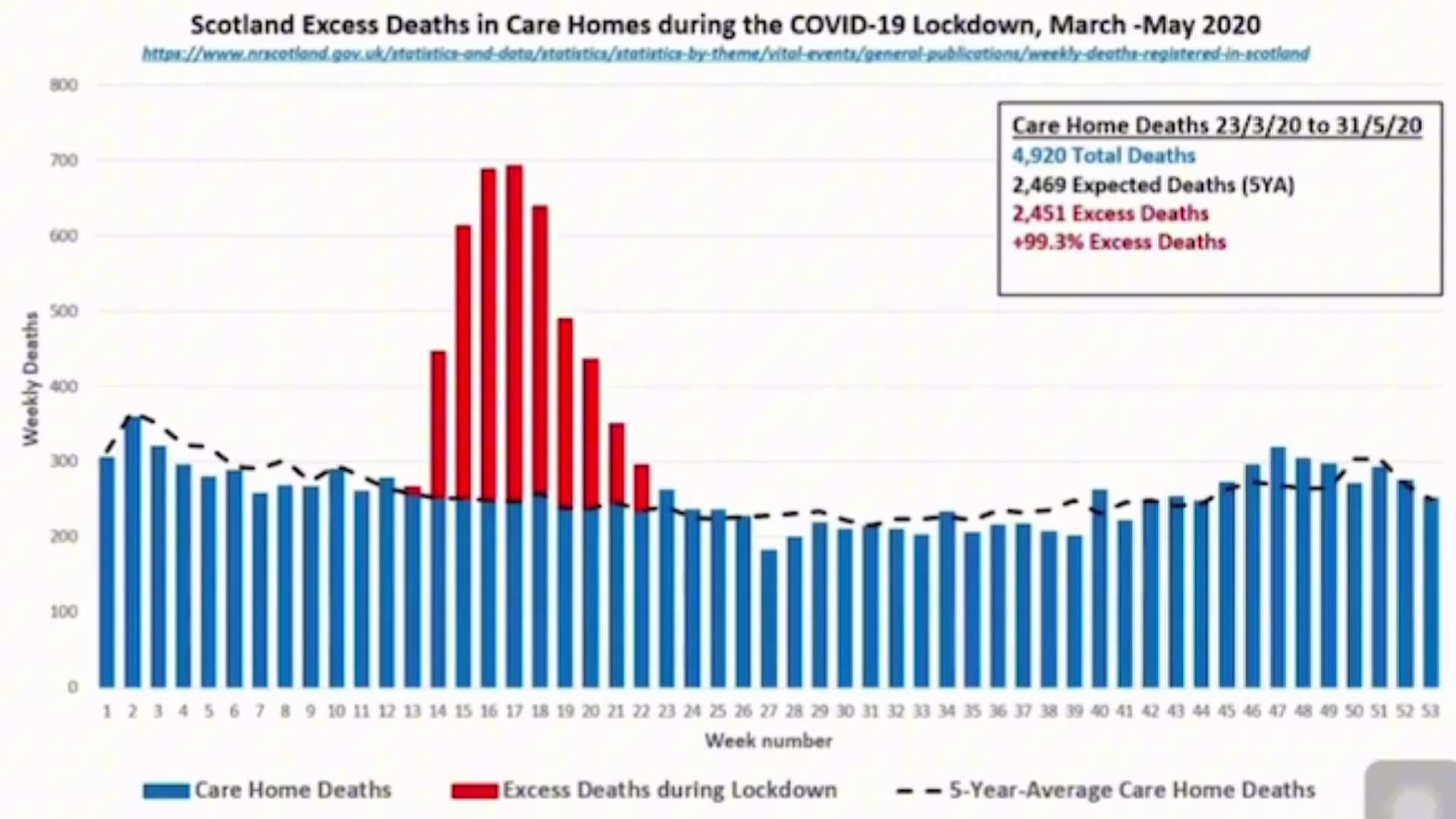
MAKE THIS VIRAL The Moment Witnesses Broke Their Silence on Scotland's End-Of-Life Care Protocols During Covid: What Really Happened... "Regardless of what the residents symptoms were, they were prescribed just in case medication (midazolam and morphine). We really struggled." via https://www.youtube.com/live/owk3_fQjlJw?si=0qwlwAZ5VO6HxQhm https://gettr.com/post/p32tpi172bf


@liz_churchill10 - Liz Churchill
ALL of the ‘Covid Crimes’ are explained accurately and thoroughly by the great Dr. David Martin @DrDMartinWorld in the below interview. Please watch this important video. https://t.co/p6NOk9OXGy
@catsscareme2021 - Jessica Rojas 🇺🇸💪
Remember the nurse I was telling you about that works for my husband? We spoke again today, and she had more to say... Well, she was a traveling nurse that was in NYC during the peak. She said, "We were given a red marker and told to put a big X on the patients that were going to die. 99% were put on ventilators, even the patients that were breathing normally. They put positive patients in rooms with people who weren't positive, and many were left in their own excrement,starved, thirsty, no family allowed, no contact with the outside world at all." She said it was the most horrific experience of her life. "If a patient didn't pop up positive,they would run the test 3 or 4 more times till it came up positive—although some never did, but they called it COVID anyway." I asked, "Did you say something to your superiors?" She smirked and said, "They were the ones giving the orders." She also has myocarditis now and can no longer work as a nurse. That's why she has a part-time sitting job where she makes about a third of what she was making as a RN. She took the shots because she didn't want to lose her job. She said the hospitals killed more people than anyone will ever realize. I told her to share her story, but she's afraid they'll come for her nursing license even though her health has deteriorated so much that she will probably never work as a nurse again. Next time I see her, I'll ask if she would be willing to make a short video sharing her experience.

@HopeRising19 - NZ and the MRNA
AUSTRALIAN PUBLIC HEALTH PROFESSOR SAYS "NO I WILL NO LONGER PUBLICLY SUPPORT COVID VACCINES.... Prof Gemma Carey Public Health Academic Covid vaccine injured (link in comments) https://t.co/bYtVfejISM
@HopeRising19 - NZ and the MRNA

@MidwesternDoc - A Midwestern Doctor
🧵Nurse Erin worked in NYC at the hardest hit COVID hospital in America. She witnessed a horrifying number of needless deaths and exposed why so many people actually died. This secret recording shows how doctors would not treat patients they knew would die with anything except the standard protocols (which had a 90% fatality rate), even when she begged them to use the off-patent therapies which were saving lives around the world. This demonstrates the perverse incentives in medicine. If you do what you are supposed to, you get paid generously and never have to worry about getting in trouble, even if you kill all of your patients. In contrast, if you do the right thing and fight for your patients (saving their lives), the medical profession and the legal system will target you, even if you're the only one saving lives. Many stories like Erin's happened throughout the pandemic, but her recordings provide the critical proof of what actually happened throughout the pandemic.
@MidwesternDoc - A Midwestern Doctor
The horrific events we witnessed during COVID were a result of what began during Obamacare. To save money, hospitals no longer focus on saving everyone, rather they are paid to get everyone out as fast as possible and sacrifice the vulnerable to do so. https://www.midwesterndoctor.com/p/what-makes-hospitals-so-deadly-and

@MidwesternDoc - A Midwestern Doctor
The hundreds of COVID deaths at Elmhurst hospital were sensationalized by the media to justify the lockdowns. Here, Erin shows that the entire disaster was manmade but no one else questioned the abhorrent COVID protocols. To prevent another COVID-19, her story must be heard so we can hold those who caused it responsible.
@MidwesternDoc - A Midwestern Doctor
This resulted from medical training now only teaching doctors to follow protocols and to believe anyone the protocols don't help could never be saved. Here I show how real doctors constantly look for solutions and always find a way to help their patients. https://www.midwesterndoctor.com/p/why-do-doctors-give-up-on-patients

@MidwesternDoc - A Midwestern Doctor
Here, another nurse also shares how gross medical mismanagement killed many NYC patients. COVID hospital survival depended upon the skill of the caregivers and in many cases clueless healthcare workers killed patients. Sadly, Medicare incentivized this by paying more for deaths.
@MidwesternDoc - A Midwestern Doctor
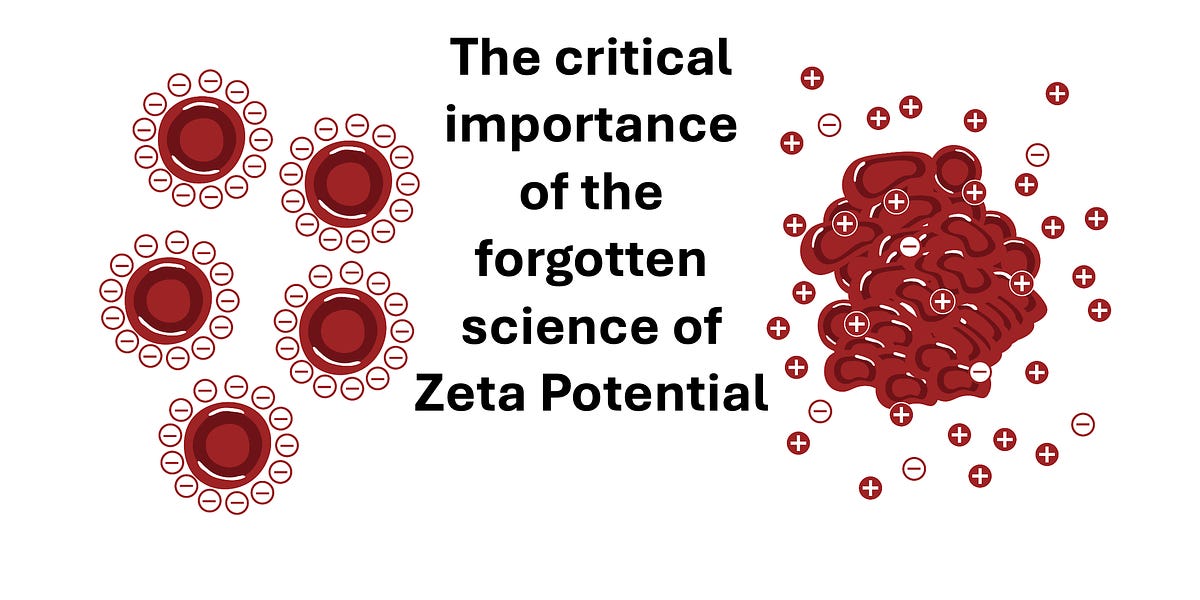
From having talked to numerous doctors in NYC, I believe the death rate there was so high because: •Medicare did not incentivize saving patients and paid more if they were put on lethal protocols or died. •Many of the people in NYC had immense psychosocial stress and pre-existing health conditions which made them much more vulnerable to COVID. •A collective fear and anxiety took over the area. Because of this, many patients went to the ER early in their illness and were aggressively put onto ventilators by panicked staff, who then accepted this was a once in a century plague and that those deaths were "innevitable." •Likewise, one of the greatest things that worsens respiratory distress is anxiety or fear, and that essentially spread like a contagion through NYC during the early days of COVID-19, causing many borderline COVID patients to go into respiratory failure. •Because the doctors were terrified of COVID (as they saw coworkers die), they avoided the COVID patients (e.g., putting them alone in ICU rooms), which caused the patients to get less care and attention than they needed. •The media (and the DNC) greatly benefitted from stoking as much fear about the pandemic, so the people in NYC were effectively sacrificed to cement a belief is this national emergency. •There was such a large surge in patients requiring COVID-19 care that many of the healthcare workers who treated them were simply not prepared to handle critically ill patients, resulting in them grossly mismanaging the cases and killing the patients (as these nurses attested). •The COVID-19 quarantine protocols kept COVID-19 patients from having patient advocates who would normally prevent these incidents. •Because the US medical system ignored what was happening in China and then Europe, they were grossly unprepared for COVID-19. As such, the early treatment protocols they used were totally inappropriate for the disease (e.g., it took a long time for American medicine to recognize steroids helped). •One of the unusual aspects of COVID-19 is that its spike protein has a high positive charge density that collapses the physiologic zeta potential of the body, causing microclots throughout the body. Because of this, it rapidly obstructs the circulation in smaller blood vessels which can't pass those microclots (whereas larger vessels like the ones you require to stay alive are relatively unaffected). Since blood oxygen levels are normally measured in the fingers (which lost much of their blood supply), this resulted in COVID patients having very "low" blood oxygen levels, which in standard ICU care requires immediately intubating the patients to pre-emept respiratory failure. Over time, ICU docs realized that COVID-19 patients with low O2 sats were actually fine (e.g., "happy hypoxics") and because less aggressive with intubating them (as it was then clear the risks of ventilating them greatly outweighed the benefits), but during the early waves this was not known. I explain the final point (zeta potential and COVID-19) in more detail here (and how it relates to vaccine injuries): https://www.midwesterndoctor.com/p/what-makes-all-vaccines-so-dangerous
@MidwesternDoc - A Midwestern Doctor
A key issue with COVID was that the spike protein caused microclotting. Since blood oxygen is measured in the fingers (which get blocked by microclots), patients who were fine appeared to be critically hypoxic and were erroneously intubated, killing them. https://www.midwesterndoctor.com/p/what-makes-all-vaccines-so-dangerous

@toobaffled - “Sudden And Unexpected”
Covid Vaccine Injured Woman Calls Out For Help As The Many Injured Are Dying A registered nurse that goes by Lyndsey, RN on X gives an emotional update with what she and other "vaccine" injured people are going through. "We need help. There are so many of us that are injured. We are dying. If you guys want your research, you have to come get us. You have to seek us out. Tell us you want to research us. If not, we're not going to be alive much longer." Lyndsey, RN🔗 Mhttps://x.com/houselyndseyrn/status/1873503257429241985?s=46&t=Maabt7-maA9Mmu3jjuQH-w

@newstart_2024 - Camus
Unvaccinated Nurse shares the horrific truth of what they are seeing in hospitals Since 2021, her hospital is witnessing an unprecedented collapse in public health: - Heart & kidney issues are "out of control." - Diabetes in new patients is up 75%. - "Turbo cancers," mysterious pneumonia, and shocking strokes are "through the roof." - Patients are suffering from bizarre symptoms, including bleeding behind the eyes and wounds that refuse to heal. "People are dying at a rate that blows my ever-loving mind," she states, after 16 years of service. "I've never seen people die like this. Ever." The scariest part? The healthcare system is buckling under the weight of caring for the millions affected. This is a silent crisis, and it's just beginning.

@sophiadahl1 - Sophia Dahl
Registered Nurse Gail Macrae: "These Covid protocols... [were] causing these patients to go into organ failure.... People say their loved ones died of Covid. I'm sorry, but that's not the way it went down. People actually died in the hospital from the protocols."‼️🙏👇 Full Video 👇👇 https://youtu.be/in7anL-1EtE?si=uxfUWPZQqT7GbkA4

@DianaT192 - Diana PATRIOTS ARE UNITED❤️🇺🇸❤️🙏
This nurse tells the truths about our horrible medical system ! https://t.co/qgR0d2ERlo

@ValerieAnne1970 - Valerie Anne Smith
Deborah Conrad, Hospital PA, was fired mid-shift for doing her legal duty—reporting Covid vaccine injuries to VAERS. She was thrown out of the hospital for telling the truth about suppressed data. This is what happens when medicine serves Big Pharma instead of patients. https://t.co/63UgOLmuQ4
@ValerieAnne1970 - Valerie Anne Smith
video credit: @AFLDSorg
@MidwesternDoc - A Midwestern Doctor
🧵Nurse Erin worked in NYC at the hardest hit COVID hospital in America. She witnessed a horrifying number of needless deaths and exposed why so many people actually died. This secret recording shows how doctors would not treat patients they knew would die with anything except the standard protocols (which had a 90% fatality rate), even when she begged them to use the off-patent therapies which were saving lives around the world. This demonstrates the perverse incentives in medicine. If you do what you are supposed to, you get paid generously and never have to worry about getting in trouble, even if you kill all of your patients. In contrast, if you do the right thing and fight for your patients (saving their lives), the medical profession and the legal system will target you, even if you're the only one saving lives. Many stories like Erin's happened throughout the pandemic, but her recordings provide the critical proof of what actually happened throughout the pandemic.